

Abstract
Objective: Serotonergic dysfunction is considered to be involved in the pathophysiology of borderline personality disorder (BPD). The aim of this study was to investigate serotonin transporter availability in patients with BPD as a marker of the central serotonergic system.
Methods: Eight unmedicated patients with BPD and 9 healthy control subjects received single photon emission computed tomography (SPECT) 4 hours after injection of 185 MBq [I-123] ADAM (2-([2-([dimethylamino]methyl)phenyl]thio)). As a measure of brain serotonin transporter (SERT) availability, ratios of specific-to-nonspecific [I-123] ADAM binding for the brainstem and hypothalamus were calculated with an occipital reference. Levels of impulsiveness and depressive symptoms were assessed with the Barratt Impulsiveness Scale and the Beck Depression Inventory.
Results: Mean specific-to-nonspecific ratios showed a 43% higher brainstem and a 12% higher hypothalamus ADAM binding in patients, compared with control subjects. We found significant correlations of ADAM binding with both age and impulsiveness but not depression. Associations of BIS scores with ADAM binding remained significant after controlling for age and depression (r = 0.69, p < 0.01).
Conclusion: The study provides evidence of a serotonergic dysfunction in patients with BPD and suggests a serotonergic component in the pathophysiology of the disorder. SERT binding reflected the level of impulsiveness as a common feature in BPD.
Introduction
Borderline personality disorder (BPD) is a severe and persistent mental condition characterized by marked impulsiveness, aggressive and auto aggressive behaviour and a wide range of unstable patterns of interpersonal relationships; self-image and affect regulation are core features of this disorder. 1,2 BPD is one of the most common disorders in the clinical setting, with an estimated prevalence of up to 10% of psychiatric outpatients and up to 20% of inpatients.3 Impulsivity is significantly associated with the lifetime number of suicide attempts,4 and the mortality rate by suicide is almost 10%.5 The etiology of BPD is poorly understood; however, alterations of emotional regulatory systems within various brain regions and a dysfunction of central serotonergic activity seem to be involved in the underlying neurobiological mechanisms.6,7 Impulsiveness is a central feature of BPD,2 and there is increasing evidence from cerebrospinal fluid (CSF), electrophysiological and pharmacological challenge studies that impulsiveness is modulated and controlled by the serotonergic system.8–11
In recent years, neuroimaging studies with single photon emission computed tomography (SPECT) or positron emission tomography (PET) and serotonergic radioligands have been performed in subjects with impulsive behaviour to directly assess brain serotonergic parameters, such as pre- or postsynaptic serotonin transporters (SERT) or serotonin receptors.12–14
Until recently, the possibilities in imaging the SERT with SPECT in the living human brain were limited because of the lack of highly selective SERT radioligands. [I-123]β-CIT used so far for imaging the SERT also binds to the dopamine transporter with high affinity.15 Recently, with [I-123] ADAM (2-([2-([dimethylamino]methyl)phenyl]thio)-5-I-123-iodophenylamine), a new highly selective SERT ligand has been presented.16,17 [I-123] ADAM has a more than 1000-fold higher selectivity for the SERT than for the norepinephrine transporter and the dopamine transporter. Previous studies with this tracer have proven its ability to visualize, detect and quantify serotonergic dysfunction in patients with depression.18,19
Here we used SPECT and this novel SPECT ligand to assess brainstem and hypothalamus SERT availability in unmedicated patients with BPD and in healthy control subjects. We hypothesized that ADAM SERT binding is different between patients and control subjects, providing in vivo evidence of central serotonergic alterations in BPD. Based on evidence showing that impulsiveness is associated with central serotonergic dysfunction, we further investigated whether impulsiveness, as assessed by self-report questionnaires in the whole study population, is associated with SERT availability, irrespective of the diagnosis.
Methods
The study was reviewed and approved by the local ethics committee of the Ludwig–Maximilians University of Munich and by the federal regulatory authorities regarding the use of radioactive agents. All subjects gave written informed consent for participation in this study, after the procedures had been fully explained by the research physicians of both the departments of psychiatry and nuclear medicine.
The study population comprised 8 female patients with BPD, ranging in age from 18 to 34 years (mean 23.2, standard deviation [SD] 5.16 yr) and 9 female healthy control subjects (21–31 yr, mean 25.9, SD 3.49 yr). The control subjects, mainly recruited from students and hospital personnel, were free of any previous or current neuropsychiatric disorders, exposure to psychotropic medication or other substances known to affect the brain serotonin system, or a family history of neurological or psychiatric diseases, as assessed by medical history, structured interviews and checklists adopted from the structured clinical interview for the DSM-IV (German version).20
We consecutively recruited the patients, whom experienced research psychiatrists diagnosed. Patients had to fulfill the criteria for BPD according to the Diagnostic and statistical manual of mental disorders, fourth edition (DSM-IV 301.83),2,20 and the Diagnostic Interview for BPD (DIB).21 Exclusion criteria were age below 18 or above 40 years; presence of current or lifetime criteria for schizophrenia, schizoaffective disorder, bipolar disorder, current eating disorder, alcohol or substance use disorder; presence of a current major depressive episode; and any other medical or neurological illnesses. The patients had to be free of any psychotropic medication for at least 12 weeks. Six patients were drug naive. Two patients reported a transient medication with benzodiazepines in their history, both were currently off medication for more than 6 months and more than 1 year, respectively. All subjects were required to have a negative urine pregnancy test, performed immediately before the application of the radiotracer. Six patients and 4 control subjects were smokers; 5 and 4 subjects, respectively, were taking oral contraceptives.
Clinical assessments
We estimated impulsiveness with the Barratt Impulsiveness Scale (BIS),22 a 34-item self report questionnaire designed to assess subjects’ levels of impulsiveness. The BIS has been established in research on impulsive behaviour. The BIS total score provides a measure of overall impulsiveness, widely used in neurobiological studies, and has been found to be increased in populations such as borderline or antisocial personality disorder. The BIS consists of 3 subscales, derived by factor analysis, assessing attentional or cognitive impulsiveness (AI; not focusing on the task at hand), motor impulsiveness (MI; acting without thinking) and nonplanning impulsiveness (NI; not planning and thinking carefully).
We assessed depressive symptoms as a common feature cooccurring in people with BPD,23 using the Beck Depression Inventory (BDI), a widely used 21-item self-report rating inventory measuring attitudes and symptoms characteristic of depression.24
SPECT imaging
Each subject received a standardized bolus injection of 185 MBq [I-123] ADAM (Map Medical, Tikkakoski, Finland). Data were acquired with a triple-headed gamma camera (Philips Prism 3000, Philips Medical Systems, Bothell, Wash.), using low-energy, high-resolution fan beam collimators. Stringent quality control of the camera system was assured.
All scans were acquired 4 hours after intravenous injection of the radiopharmaceutical. This time frame is considered optimal for semiquantification of specific radiotracer binding.25,26 A 128 × 128 matrix was used for all acquisitions. The rotational radius was minimized to less than 13 cm in all cases. A total of 120 projections were acquired at 60 second per view, with the camera heads following a circular orbit, resulting in a total scan time of 43 minutes. The projection data were checked visually for patient motion, using the cine display and sinograms provided by the software of the camera manufacturer (Odyssey-FX software, Philips Medical Systems, Bothell, Wash.).
SPECT data were reconstructed by backprojection (ramp filter), filtered with a Butterworth 3D postfilter (0.6 cycles/cm, 5th order) and corrected for attenuation according to Chang’s method (μ = 0.11/cm, value confirmed from previous phantom measurements, elliptic fitting with separate contours for each slice) as outlined in the European Association of Nuclear Medicine (EANM) procedure guidelines for brain neurotransmission SPECT.27
Quantitative evaluation
We evaluated images with a semi-automated quantification software, based on a modified version of the Brain Analysis Software (BRASS, version 3.4.4), running on a Hermes workstation (Hermes Medical Solutions, Stockholm, Sweden). It is based on a multistep registration of individual patient studies to a template of healthy control subjects. For this software approach, a template and a 3D volume of interest map were specifically created for [I-123] ADAM scans.
A SPECT template (2 mm isotropic voxel size) was created with the images of 20 healthy control subjects acquired in previous research projects approved by the ethics committee. In 4 subjects, additional MRI images (sagittal MPRAGE sequence, 1 × 1 × 1-mm voxel size) were obtained with fiducial MRI/SPECT markers (nitroglycerin pills injected with approximately 10 kBq I-123) attached, which served as a basis for the coregistration and which were used to align images according to the Talairach space (Fig. 1A). Based on these MRI scans, a standardized 3D volume of interest (VOI) map (Fig. 1B) was created, including regions for the brain stem (456 voxels), the hypothalamus (604 voxels) and an occipital reference region (9008 voxels). The target regions for the analyses (hypothalamus and brain stem) were selected in accordance with previous reports of the [I-123] ADAM distribution in the brain18,25 and represent the SERT-rich regions, particularly the raphe nuclei. The method follows the previously developed automated quantification approach for dopamine transporter SPECT images.28

[I-123] ADAM (2-([2-([dimethylamino]methyl)phenyl]thio)) SPECT template used for the automated semi-quantification. Image fusion (A) with the MRI and the 3D volume of interest map (B) derived from the MRI scan. Delineation of the region of interest (brainstem, hypothalamus) and the nonspecific occipital reference region.
Individual scans of patients and healthy control subjects were then registered to the [I-123] ADAM template by applying an automated fitting algorithm. The software registers individual studies to the mean template, adjusting 9 parameters (3 each for rotation, translation and anisotropic scaling) of an alignment transformation matrix, using principal axes technique and an iterative, simplex algorithm to maximize normalized mutual information, a measure of similarity between the transformed individual study and the template.29,30 After successful registration, the standardized 3D VOI map is applied to each scan. Owing to variation in anatomy, the brain stem and hypothalamus regions were adjusted manually to match the corresponding structures where necessary.
Based on the mean counts per voxel in the respective volumes of interest, the specific radiotracer binding for the brain stem was calculated by applying the following formula:

Statistics
Statistical analyses were performed and data were tested for normal distribution (one sample Kolmogorov–Smirnov test) and equality of variance (Levene test). Means and SDs were calculated as descriptive analyses of clinical and imaging variables. Group differences were compared with the unpaired t test (2-sided) for independent samples. To control for the effects of clinical symptoms (impulsiveness, depression), we performed analyses of covariance (ANCOVA) with age adjusted ADAM binding as an dependent variable and impulsiveness or depression scores as covariates. Adjustments for the effects of age were performed by a linear regression model with age as the independent variable. Correlations of imaging data, age and clinical variables were assessed by calculating Pearson’s correlation coefficients, and we computed partial correlations to control for the effects of age or clinical variables. The p < 0.05 level was considered statistically significant.
Results
Table 1 shows the demographic and clinical data of the study population. Statistical analyses revealed a normal distribution and homogeneity of variances of demographic (age) and imaging data in either group (Kolmogorov–Smirnov test, Levene test, respectively, nonsignificant). Patients and control subjects did not differ significantly in mean age (t15 = 1.3, p = 0.22). Overall impulsiveness as assessed by the BIS total score ranged from 65 to 97 (mean 83.75 [SD 9.63]) in the patient group and was statistically significantly higher (t15 = −5.81, p < 0.01), compared with the group of healthy control subjects (range 50–70, mean 60.11 [SD 7.08]). The differences were also significant for each BIS subscore, for example, AI, MI and NI (t15 = −5.27, p < 0.01; t15 = −7.38, p < 0.01; and t15 = −2.68, p < 0.05, respectively).
Demographic, clinical, and SPECT imaging data of healthy female control subjects and female patients with borderline personality disorder
Cooccurring depression as assessed by the BDI was present in the group of patients with a mean score of 27.71 (SD 10.67) (range 14–44). In the control group, BDI scores ranged from 0 to 6, with a mean (SD) of 1.56 (2.13) (difference statistically significant, t15 = −6.39, p < 0.01).
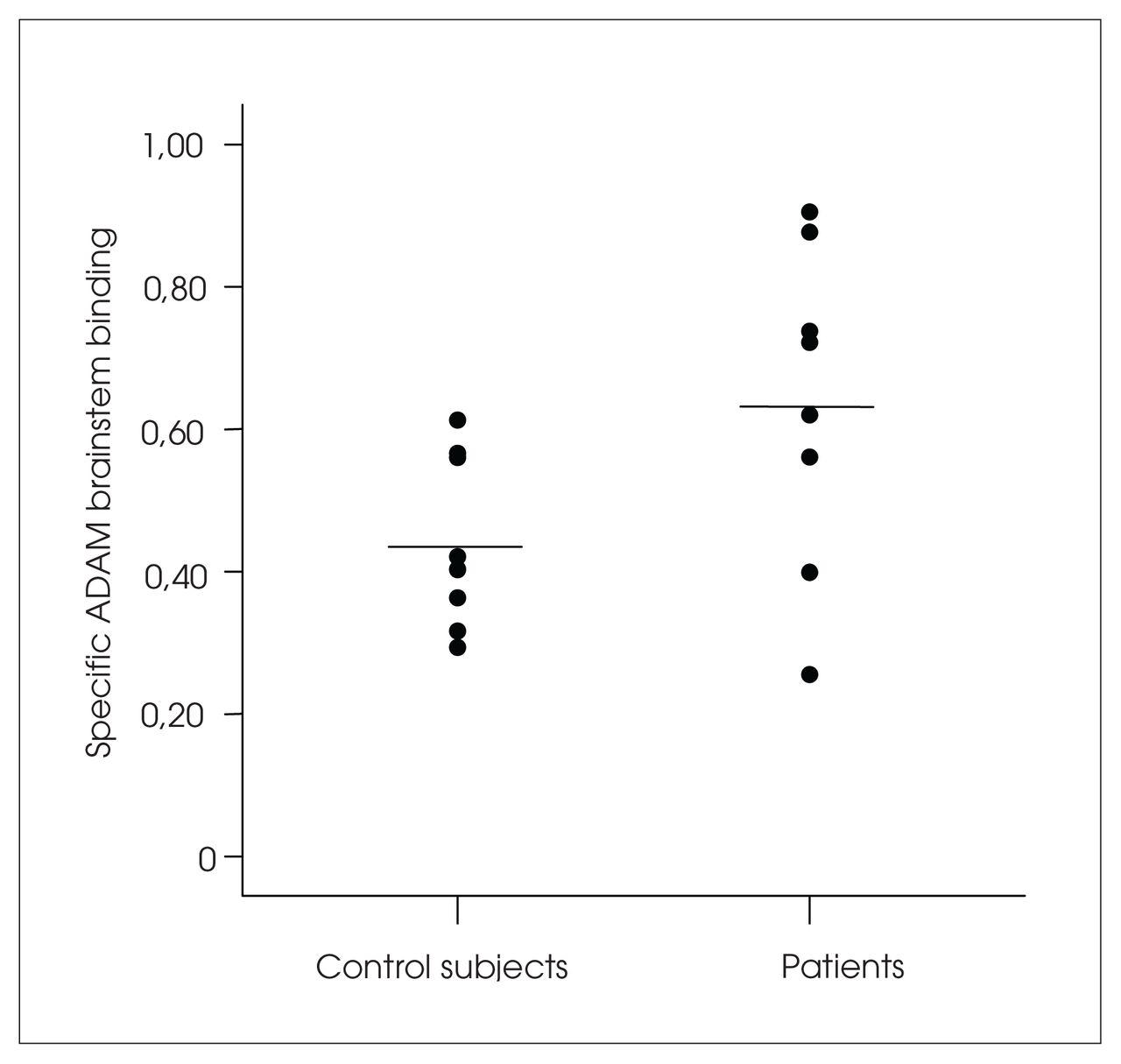
Four hours after intravenous injection of the radio-tracer, specific-to-nonspecific ratios of [I-123] ADAM binding to the brainstem and the hypothalamus region ranged from 0.29 to 0.61 and 0.77 to 1.07, respectively, in the control group and from 0.26 to 0.91 and 0.90 to 1.22, respectively, in the patient group (Fig. 2).

Specific [123-I] ADAM (2-([2-([dimethylamino]-methyl)-phenyl]thio)) brainstem binding in healthy control subjects and patients with borderline personality disorder.
The mean specific brainstem ADAM binding was significantly different between the groups, with a 43% higher mean brainstem binding in the patient group (0.63 [SD 0.23] v. 0.44 [SD 0.12]; t15 = −2.31, p = 0.035, Fig. 2). Within the hypothalamus, the mean specific ADAM binding was 1.05 (SD 0.11) in the patient group, which was about 12% higher, compared with the control subjects (0.94 [SD 0.10]). This difference also reached statistical significance (t15 = −2.14, p = 0.049).
The differences between the groups remained statistically significant when we adjusted the SPECT data for age, using a linear regression model and controlled for the effects of covariates such as clinical symptom scores (i.e., impulsiveness and depression as assessed by the BIS and BDI, respectively) by analysis of covariance (ANCOVA), with ADAM brainstem binding as the dependent variable: F1,13 = 5.27, p = 0.04; with ADAM hypothalamus binding as the dependent variable: F1,13 = 7.12, p = 0.02.
Regarding the whole study population, correlation analyses revealed both significant correlations between age and ADAM brainstem and hypothalamus binding (r15 = −0.69, p = 0.002 and r15 = −0.63, p = 0.007, respectively) and impulsiveness and ADAM brainstem and hypothalamus binding (r15 = 0.62, p = 0.009; r15 = 0.49, p = 0.04). However, when looking at the patient and control groups separately, correlations between impulsiveness and SPECT variables failed significance. There were no significant correlations between SPECT variables and depression scores, neither in the whole sample nor in the group of patients (Fig. 3 and Fig. 4). The association between impulsiveness and ADAM brainstem binding in the whole sample remained significant after controlling for the cofactors age and BDI scores, using partial correlations (r13 = 0.69, p = 0.007).

Correlation of [123-I] ADAM (2-([2-([dimethylamino]-methyl)phenyl]thio)) brainstem binding with the total score of the Barratt Impulsiveness Scale for the entire study population (patients = filled circles, control subjects = open circles).
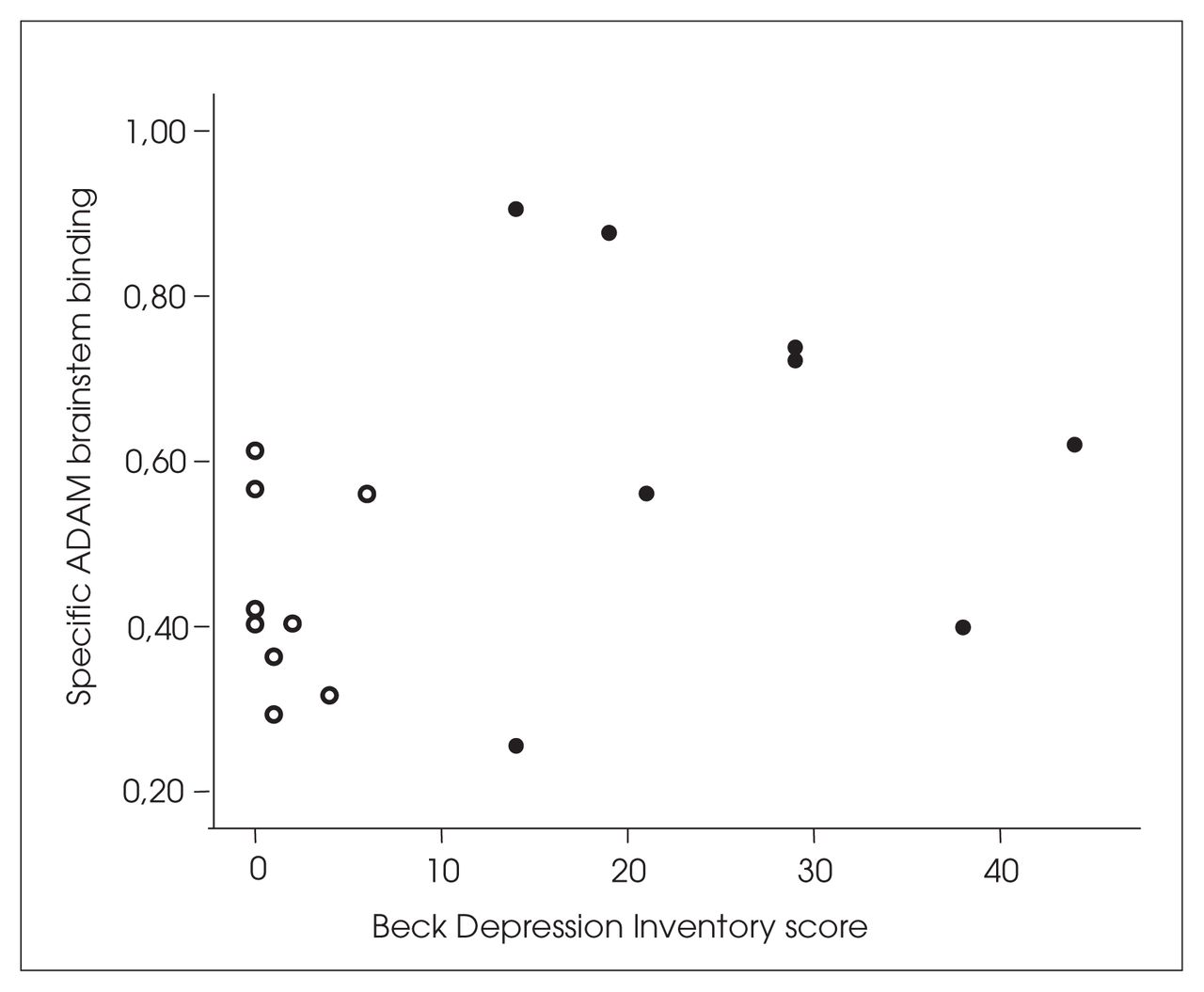
Scatterplot of [123-I] ADAM (2-([2-([dimethylamino]-methyl)phenyl]thio)) brainstem binding and the scores of the Beck Depression Inventory for the study population (patients = filled circles, control subjects = open circles).
Discussion
To our knowledge, this is the first study of patients with BPD using SPECT and the novel SERT ligand [I-123] ADAM to assess central SERT availability in vivo in this population. The central serotonergic system is considered to play a key role in the pathogenesis of BPD.9,10,31 Current pharmacological treatment is therefore primarily based on selective serotonin reuptake inhibitors (SSRIs), which have proven successful for various symptom constellations in these patients.
Our data showed significantly higher SERT binding in patients with BPD, compared with healthy control subjects of the same sex and comparable age distribution, which strongly supports the hypothesis of a serotonergic dysfunction in BPD. The elevated ADAM binding could reflect a higher number of serotonin transporters with an increased capacity of presynaptic serotonin reuptake or be the consequence of an increased number of available binding sites, owing to decreased competition by lower endogenous serotonin levels.15,32
From earlier studies, it is known that other psychiatric disorders (e.g., major depression, bulimia, obsessive–compulsive disorder)33–35 can also be associated with a serotonergic dysfunction influencing SERT availability. Possible interference of any of these disorders with SERT binding was excluded in our subjects. Depressive symptoms as a common clinical feature in BPD23 were present in our group of patients, but unlike other studies,35,36 the respective scores were not associated with SERT availability.
Meyer and colleagues37 demonstrated a strong association of SERT availability and dysfunctional attitudes with [C-11] DASB PET. However, in a study with PET and [F-18] setoperone, the same group found significant correlations of dysfunctional attitudes and 5-HT2 binding only in patients with major depressive episodes and not in patients with long-term self-harm behaviour.38 Altogether, these findings suggest distinct neurobiological mechanisms of psychiatric symptoms in different disorders and therefore do not contradict our results.
The patients of our study were drug free and did not take any medication known to interfere with SERT uptake of the radiotracer. Since only women participated in the project, general sex differences as described in a recent study by Staley and colleagues39 can also be disregarded. We could not control for the menstrual cycle, a previously reported possible element in estrogen–serotonin interactions.40 However, the findings of a recent study with β-CIT and SPECT suggested that matching female subjects according to menstrual cycle is unnecessary, regarding serotonin and dopamine transporters.41 Similarly, the effects of smoking on SERT availability seem to be negligible in female subjects.39
Given the overlap of SERT availability between the patients and the control subjects in our study, correlation analyses were performed for the entire study population as a dimensional, symptom-based approach to assess the effects of single personality or clinical items. There were significant associations of the scores of the BIS and age, but not depression scores with specific radiotracer binding to the SERT. The effects of impulsiveness remained statistically significant even when controlling for age and depression scores in partial correlation analyses. Similarly, BIS scores and age, but not BDI scores, contributed in linear regression analyses to predict SERT binding.
Increased impulsiveness was associated with higher SERT availability, with the highest correlation being observed with the BIS motor and attentional subscales. This supports previous observations showing that biochemical findings in BPD patients were attributed to aggression scores, impulsiveness and irritability.8,10
Serotonergic dysfunction has also been shown in other psychiatric patient populations, such as suicidal patients14,42 and patients with violent or aggressive behaviour. 12,13,43 In light of these findings, the higher radiotracer binding to the SERT in our patients probably reflects the level of impulsiveness as a common feature in several psychiatric disorders rather than representing a factor specific for BPD.
With SPECT and the nonspecific monoamine transporter ligand [I-123] β-CIT, Tiihonen and colleagues12 have shown lower β-CIT midbrain binding in impulsive violent offenders indicating reduced SERT availability, compared with control subjects. Sekine and colleagues44 presented a negative correlation of aggressiveness and SERT binding of the SERT-specific PET tracer [C-11] McN 5652 in many brain regions, including the cerebral cortex, cerebellar cortex and basal ganglia, but not the midbrain area, in abstinent patients with methamphetamine abuse.
At first glance, these results appear contrary to our findings; however, the patient populations of both mentioned studies consisted of subjects with neurotoxic substance abuse. The latter may not only induce selective damage to the serotonergic system, but also affect dopaminergic, glutamatergic and GABA-ergic neurons.
The work of Sekine and colleagues44 demonstrates the global impact of methamphetamine abuse on SERT binding, affecting areas with low SERT availability (e.g., the cerebellum). The patient population included by Tiihonen and colleagues12 consisted primarily of alcohol-dependent patients committing violent offenses under the influence of alcohol; most of these subjects also had either antisocial or mixed-type personality disorder. Aggression and impulsiveness in these studies may therefore result from mechanisms different from those in our unmedicated and partially drug-naive patients with BPD.
Frankle and colleagues13 studied the SERT distribution in subjects with impulsive aggression using PET and [C-11] McN 5652. The authors found significantly reduced SERT availability in the left anterior cingulate cortex of individuals with impulsive aggression, compared with healthy control subjects. In contrast, no significant differences between patients and control subjects could be shown for the midbrain region. Compared with our findings, the latter could be explained by concomitant mood disorders retrospectively diagnosed in many of the patients examined, possibly resulting in a reduction of SERT availability in the midbrain area.33 This might have hampered the detection of a potential midbrain SERT alteration. The presence of depressive symptoms in our patients might have influenced the imaging data, although our findings remained stable when we controlled for these variables.
Some methodological limitations of our study need to be addressed. First, the number of subjects included is limited, possibly reducing the accuracy of multifactorial analyses (linear regression, analysis of variance). Second, there was no MRI coregistration for the placement of VOIs to identify brain regions with low activity (the anatomically poorly circumscribed SERT-enriched regions in the diencephalon, midbrain or brainstem) more accurately, as previously described.25 However, in accordance with other groups,33,34 we chose standardized templates with fixed sizes for the 3D volumes of interest to reduce variance. Automated registration algorithms provided a high level of observer independence. 28,30 We also used the occipital cortex for semiquantification, an area not entirely free of SERT expression,45 instead of the cerebellar cortex with lower specific radiotracer binding. This seems justified in light of parallel radiotracer kinetics in the occipital cortex and the cerebellum.25 Owing to the lack of morphological information in ADAM images, accurate attenuation correction in the cerebellum is critical, and the use of a cerebellar reference region might introduce additional sources of error.
Although our findings are preliminary and are derived from a limited cohort of subjects, they suggest a direct alteration of the serotonergic system in patients with BPD. The marked elevation of SERT availability, and a particular correlation of SERT data with the cardinal clinical feature “impulsiveness,” strengthens the hypothesis of the serotonergic system as a pathophysiological key role in patients with BPD. Prospective SPECT studies with a higher number of subjects are warranted to further validate our data. Data obtained during follow-up of patients under pharmacological or psychological treatments would be of particular interest.
Acknowledgements
This work was supported by a grant from the Faculty of Medicine, Ludwig–Maximilians University of Munich (FöFoLe No. 253), and was part of Nadine Schaaff’s doctoral thesis.
Footnotes
Medical subject headings: borderline personality disorder; impulsive behaviour; serotonin transporter; single photon emission computed tomography.
Competing interests: Dr. Tatsch received travel assistance and an educational grant for a lunch symposium during an EANM meeting.
Contributors: Drs. Koch, Schaaff, Pöpperl, Juckel, Möller, Hegerl, Tatsch and Pogarell designed the study. Drs. Koch, Schaaff, Pöpperl, Reicherzer, Ehmer-von Geiso and Pogarell aquired the data, which Drs. Koch, Schaaff, Pöpperl, Mulert, Tatsch and Pogarell analyzed. Drs. Koch and Schaaff wrote the article, and Drs. Pöpperl, Mulert, Juckel, Reicherzer, Ehmer-von Geiso, Möller, Hegerl, Tatsch and Pogarell revised it. All authors gave final approval for the article to be published.
- Received October 5, 2006.
- Revision received December 1, 2006.
- Revision received December 22, 2006.
- Accepted December 22, 2006.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.