

More than 15% of the world’s burden of disease is attributable to interlocking neurologic and psychiatric (neuropsychiatric) disorders; these syndromes include mood disorders, schizophrenia, addiction, dementia, epilepsy and chronic pain disorders.1 Neuropsychiatric disorders associated with HIV infection represent the convergence of a major global infectious epidemic with nervous system disease, resulting in substantial morbidity and mortality, especially as the disease progresses to AIDS. HIV directly infects and injures the central and peripheral nervous systems, culminating in a wide spectrum of neuropsychiatric disorders (collectively termed neuroAIDS), including neurocognitive disorders such as HIV-associated dementia, minor neurocognitive disorder, mania/psychosis, anxiety, depression, seizures, and myelopathy and neuropathy with accompanying chronic neuropathic pain and physical disabilities (Fig. 1). In fact, HIV entry into the nervous system (neuroinvasion) occurs early after primary infection but persists throughout the disease course because the virus chronically infects glial cells (neurotropism) and has ensuing potential for nervous system disease (neurovirulence). However, only a subset of people with HIV exhibit nervous system disease, indicating selective vulnerability to a neuropsychiatric phenotype (neurosusceptiblity) caused by HIV, defined by age, level of concurrent immunosuppression, comorbidities and both host and virus genetic diversities.2 These neuropsychiatric disorders are associated with diminished quality of life,3 increased health care costs4 and reduced survival.5 Several of these disorders are also apparent in children with HIV who also have developmental delay.6 In addition, systemic immunosuppression increases the risk, particularly among adults, of opportunistic processes within the nervous system, including progressive multifocal leukoencephalopathy, toxoplasmic encephalitis, cryptococcal and tuberculous meningitis and primary central nervous system lymphoma associated with seizures, physical and cognitive disabilities, psychosis and mood disorders.
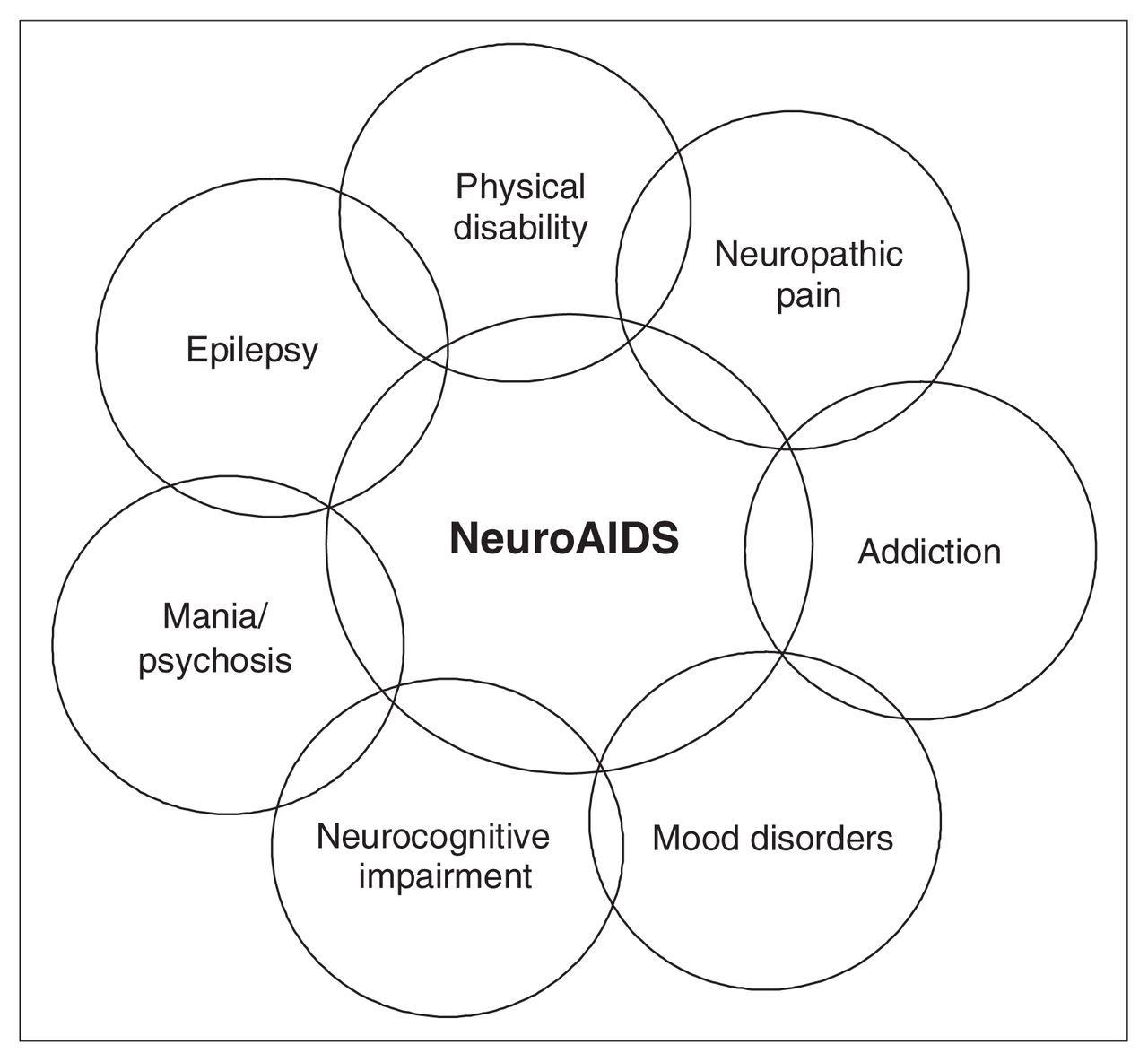
Overlap of NeuroAIDS-associated neuropsychiatric phenotypes. The individual disease phenotypes depend on the affected anatomic site, the stage of disease including premorbid status, intercurrent illness (immunosuppression), age and, in some cases, concurrent therapies.
With the advent and increasing global use of combination antiretroviral therapy, there has been a reduction in the frequency and severity of neuropsychiatric disorders classically described in HIV infection, together with improved immune status and a reduced incidence of opportunistic disorders. Likewise, the quality of life and survival time of individuals with HIV/AIDS have increased steadily with greater availability of combination antiretroviral therapy, leading to improved nervous system health and function.7 Despite this progress, recent data reveal that neuropsychiatric complications still occur in as many as 50% of people with HIV.5 Although the spectrum of HIV-related neuropsychiatric disease has changed, even these newer assessments of disease prevalence might underestimate the true burden of neuropsychiatric disease.
The spectrum of neuropsychiatric disease among those infected with HIV is captured by stratifying disorders into 3 categories:
premorbid illnesses in patients with HIV (e.g., schizophrenia, major depression, anxiety disorders, addiction, mental retardation);
illnesses directly caused by HIV infection (e.g., neurocognitive disorders, seizures, neuropathy and associated complications); and
illnesses related to the medications commonly used in the treatment of HIV (e.g., delirium, pain, anxiety).
In North America, populations at high risk for HIV include injection drug users, men having sex with men, Aboriginal peoples, youth and prisoners. Infection, in many cases, is a consequence of high-risk behaviours, including unprotected sex or injection drug use. Premorbid conditions such as addiction, mood disorders, anxiety disorders and psychosis can place individuals at greater risk for high-risk behaviours and, consequently, for HIV infection. It is important to recognize these conditions in this “at risk” population, since previous studies demonstrate that some conditions such as depression may be associated with increased progression of HIV and higher mortality.8,9 Antecedent illnesses may also affect how and when a patient seeks medical attention, adherence to medications and follow-up. Premorbid illnesses may therefore be important determinants of behaviours that influence the spread of disease. Among men with antiretroviral drug resistance, high-risk sexual activity has been associated with depression, youth, alcohol abuse and sildenafil use,10 underscoring the diversity of factors that influence the spread of HIV.
High-risk behaviours also place individuals at risk of co-infections, which may go unrecognized and have their own neuropsychiatric consequences. Among these infections, syphilis and hepatitis C virus infections are particularly important contemporary issues. Hepatitis C virus is a common coinfection with HIV and may place patients at increased risk for HIV-associated dementia11 and contribute to mortality.12 Therapies for hepatitis C virus, including pegylated interferon-α, also have neuropsychiatric effects that complicate their use in coinfected patients.13,14 Finally, it has been shown that there is a higher prevalence of smoking among people with HIV,15 which may have negative impacts on quality of life and mortality.16
The neuropsychiatric illnesses assumed to be directly caused by HIV infection are diverse and often eclipsed by overwhelming systemic medical issues, leaving the neuro-psychiatric syndromes under-diagnosed and under-treated. These illnesses include HIV-associated dementia and minor neurocognitive disorder (or HIV-associated neurocognitive disorders), painful distal sensory polyneuropathy, vacuolar myelopathy and seizures.5,7,17 The underlying neurovirulent mechanisms for these disorders are thought to involve HIV infection of microglia and astrocytes (not neurons or oligo-dendendrocytes) and have ensuing direct neurotoxic effects mediated by induced host-encoded molecules (e.g., cytokines, proteases, reactive oxygen species, eicosanoids, excitotoxic amino acids) and neurotoxic actions exerted by virus-encoded proteins (e.g., gp120, Vpr, Tat) on proximate neurons.18 However, the literature increasingly reveals that there is an under-recognized and under-treated burden of mental health impairment19 that likely affects the quality of life, employment and survival of patients with HIV. This is complicated further by the lack of evidence on how best to treat such impairment in a population where particular attention needs to be paid to side effects and drug interactions.20 Many people with HIV are now living longer than 20 years after initial infection — long after AIDS has developed.21 The mental health consequences of living with any chronic medical illness must also be considered.22
Combination antiretroviral therapy has expanded such that there now exist more than 25 approved antiretroviral drugs with a multitude of options for therapy using several drug classes and simplified once-daily regimens. Different drug regimens, however, have varying degrees of central nervous system penetrance. Thus, the central nervous system may serve as a reservoir for HIV. Treatment may not provide complete protection against nervous system damage in HIV infection. Despite this, several studies have failed to show differences in progression and treatment of HIV-associated dementia between different therapy regimens.23,24 Treatment with combination antiretroviral therapy also places the individual, especially those with very low CD4+ lymphocyte counts, at risk for immune reconstitution inflammatory syndrome. This syndrome seemingly results from the restitution of the individual’s immune system when combination anti-retroviral therapy is initiated and has a host of documented neuropsychiatric sequelae.25,26 Neuroimmune reconstitution inflammatory syndrome has recently been recognized in the central nervous system and may be associated with neurotoxic CD8+ T cells infiltrating the brain to cause seizures, confusion and physical disabilities.25
The medications used in the treatment of HIV also have their own associated side effects, of which some are neuropsychiatric. Efavirenz is a non-nucleoside reverse transcriptase inhibitor commonly used to treat HIV. It is associated with acute central nervous system side effects in 50% of patients and has neuropsychiatric side effects when used chronically.27 Several of the antiretroviral drugs cause distal sensory neuropathy associated with neuropathic pain, but fortunately many of these drugs (e.g., didanosine, indinavir) are no longer or rarely used. However, stavudine (d4T) is part of the regimen recommended by the World Health Organization for widespread global use. There is increasing evidence of hypertension and diabetes in people with HIV. In part, this is likely due to their prolonged survival and aging, but hyperlipidemia, insulin resistance and diabetes are also recognized side effects of protease inhibitors.28 It remains to be seen how hypertension and diabetes will ultimately affect the development of associated conditions such as vascular dementia and stroke in this population. Finally, although some evidence is being accumulated, little is known about how HIV therapies interact with many of the therapies commonly prescribed to treat neuropsychiatric disorders. The importance of this is highlighted in a recently published case of bipolar disorder being exacerbated by an interaction between lopinavir/ritonavir and valproic acid.29
In summary, among individuals infected with HIV, there is a broad and burgeoning spectrum of common neuropsychiatric syndromes that are evident at all ages and involve premorbid disorders, direct HIV-induced disorders and conditions related to HIV treatments (Fig. 1). The pathobiological mechanisms of these disorders remain ill-defined and the available treatments are limited. Prolonged survival among people with HIV owing to effective combination antiretroviral therapies also leads to the possibility of previously unrecognized complications. Indeed, given the global estimates for HIV prevalence (> 33 million infected worldwide and > 1 million in North America at present) and increasing availability of combination antiretro-viral therapies, the magnitude and severity of disease related to the nervous system is a daunting challenge for already overburdened health care systems. These circumstances call for heightened awareness and vigilance among caregivers in terms of recognizing, preventing and treating these disorders because of their adverse impact on quality of life, employment, health care costs and ultimately survival. Moreover, new neuropsychiatric diseases may emerge with greater recognition of disease phenotypes associated with different HIV subtypes (clades), particularly in the developing world; the increasing prevalence of drug-resistant strains of HIV; or unanticipated consequences of new therapies. At the same time, there is increased interest in applying new technologies and approaches to studying neuropsychiatric diseases, including genomics, epigenomics, metabolomics and lipidomics, which has prompted application of systems biology to investigating neuropsychiatric disease pathogenesis.30 From these latter studies, new therapies (immunotherapies, small molecules and therapeutic vaccines) for neuropsychiatric diseases are being developed and could be implemented in conjunction with combination antiretroviral therapies in the future. These strategies might have substantial impact on the burden of neuropsychiatric disease but perhaps also on the overall HIV/AIDS epidemic given that the nervous system is a viral reservoir that remains comparatively inaccessible to immune surveillance and regulation.
Acknowledgements
The authors thank Leah DeBlock for assistance with manuscript preparation and Dr. Glen Baker for helpful discussions. F.N. is supported by Canadian Institutes of Health Research and Alberta Heritage Foundation for Medical Research Fellowships. C.P. holds a Canada Research Chair (Tier 1) in Neurological Infection and Immunity and is an Alberta Heritage Foundation for Medical Research Senior Scholar.
Footnotes
Competing interests: None declared.
References

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.