

Abstract
Background: In major depressive disorder (MDD), it is unclear to what extent structural brain changes are associated with depressive episodes or represent part of the mechanism by which the risk for illness is mediated. The aim of this study was to investigate whether structural abnormalities are related to risk for the development of MDD.
Methods: We compared healthy controls with a positive family history for MDD (HC-FHP), healthy controls with no family history of any psychiatric disease (HC-FHN) and patients with MDD. Groups were age- and sex-matched. We analyzed data from high-resolution magnetic resonance imaging using voxel-based morphometry. We performed small volume corrections for our regions of interest (hippocampus, dorsolateral [DLPFC] and dorsomedial prefrontal cortex [DMPFC], anterior cingulate cortex [ACC] and basal ganglia) using a family-wise error correction (p < 0.05) to control for multiple comparisons.
Results: There were 30 participants in the HC-FHP group, 64 in the HC-FHN group and 33 patients with MDD. The HC-FHP group had smaller right hippocampal and DLPFC grey matter volumes compared with the HC-FHN group, and even smaller right hippocampal volumes compared with patients with MDD. In addition, the HC-FHP group exhibited smaller white matter volumes in the DLPFC and left putamen but also greater volumes in 2 areas of the DMPFC compared with the HC-FHN group. Patients with MDD exhibited smaller volumes in the ACC, DMPFC, DLPFC and the basal ganglia compared with healthy controls.
Limitations: The retrospective identification of family history might result in a bias toward unidentified participants in the control group at risk for MDD, diminishing the effect size.
Conclusion: Volume reductions in the hippocampus and DLPFC might be associated with a greater risk for MDD. The HC-FHP group had smaller hippocampal volumes compared with patients with MDD, which is suggestive for neuroplastic effects of treatment. The HC-FHP group had not yet experienced a depressive episode and therefore might have been resilient and might have had some protective strategies. Whether resilience is associated with the larger white matter volumes in the DMPFC (e.g., owing to compensatory, neuroplastic remodelling mechanisms) needs to be confirmed in future studies.
Introduction
Mental disorders are a major cause of long-term disability and are a direct cause of mortality with about 800 000 individuals dying from suicide every year worldwide, a high proportion of them related to depression.1 Over the last decade, research on major depressive disorder (MDD) has shown that multiple factors may induce the illness. In this context, the interplay of genetic and environmental factors is thought to play an important role.2–4 In particular, familial depression liability and adverse events have been shown to be risk factors for the onset of the first depressive symptom.5 Moreover, the effects of adverse events on the new development of depressive episodes in individuals under familial risk have been found to be moderated by parental depression status.6 Importantly, even without the occurrence of adverse events, individuals with a familial depression liability are at greater risk for MDD, and the severity of symptoms are further increased by additional exposure to adverse events.6
Patients with MDD exhibit functional and structural brain anomalies. In particular, in vivo magnetic resonance imaging (MRI) studies have shown that key areas involved in emotional regulation, such as the hippocampus, amygdala, cingulate cortex, basal ganglia and prefrontal cortex (PFC) may go through such changes.7 A small (5%) but significant reduction in hippocampal volume is commonly found in participants with MDD,7,8 and the duration of depressive episodes has been proven to be closely associated with hippocampal volume decline in cross-sectional studies.9–11 A longitudinal study reported that grey matter volume declines in the hippocampus, anterior cingulate (ACC) and prefrontal cortices during ongoing depressive episodes.12 There is also evidence that structural changes, once emerged, have functional consequences on the outcome of the depressive illness, which becomes more severe with more hippocampal changes.13 However, whether structural changes are a result of the active disease process or whether they are present before the beginning of the acute disease remains unresolved.
Structural MRI investigations might hold promise in the early detection of structural/volumetric changes in healthy participants with a genetic risk for MDD. For example, MRI has an ability to detect both grey and white matter dysfunctions in healthy individuals with and without family history of bipolar disorder.14 Moreover, MRI might shed light on whether structural changes occur after the onset of MDD or whether they already existed before the manifestation of its symptoms.
Over the last few years, voxel-based morphometry (VBM) has become an established research method in MRI research.15 It enables the global assessment of brain structures without a priori identification of the region of interest (ROI)16 and allows the analysis of brain regions when boundaries are difficult to define.
The primary aim of the present study was to investigate whether grey/white matter volumetric hippocampal and prefrontal differences exist even between healthy adults with a family history of MDD and healthy individuals without any family history of psychiatric disorders. Our secondary purpose was to investigate the first-time putative differences between healthy participants (with and without family history of MDD) and participants with diagnosed acute MDD. In an exploratory analysis, we investigated differences between patients with a family history and those without a family history of MDD, keeping in mind that the sample size in this additional analysis was relatively small. Given the key role played by the hippocampus, the dorsolateral (DLPFC) and dorsomedial prefrontal cortices (DMPFC), ACC and the basal ganglia in the etiology of depressive disorders, we investigated putative volumetric differences in these areas as the main ROIs.
Methods
Participant recruitment
We recruited a cohort of healthy volunteers with family history of depression (HC-FHP) and healthy volunteers with no psychiatric family history (HC-FHN) from the local community via announcements and carefully screened them for medical conditions and family history. Family history of depression was assessed by a psychiatrist through a structured interview. In particular, participants were asked whether any of their first- or second-degree relatives had a diagnosed psychiatric disease, had been in treatment with antidepressant medications or electroconvulsive therapy or had attended a psychiatric service. We excluded participants in cases of movement artifacts or incomplete brain scans.
Moreover, we included patients with acute MDD directly after their first admissions to our psychiatric hospital. We documented clinical variables in patients with MDD using the 21-item Hamilton Rating Scale for Depression (HAM-D).17 It was not our primary intention to compare patients with a positive family history (MDD-FHP) and patients with a negative family history (MDD-FHN); however, we also provide these data. We used a structured written observer interview to assess medical history, trauma and other exclusion criteria for all participants. Exclusion criteria for patients with MDD and controls (HC-FHN and HC-FHP) were previous head injury with loss of consciousness, cortisol medication in their medical history, previous alcohol or substance abuse, personality disorders, neurologic diseases, age older than 65 years and comorbidity with other mental illnesses and personality disorders. Handedness was determined by the Edinburgh Handedness Inventory.18
We obtained written informed consent from all participants subsequent to a detailed description of the study. The study design was approved by the ethics committee of the Ludwig-Maximilian University, Munich, and was prepared in accordance with the ethical standards laid down in the Declaration of Helsinki.
Statistical analysis of clinical and demographic characteristics
We analyzed clinical and demographic data using SPSS-16. Differences in sex and handedness were analyzed using χ2 tests. Further, differences in age, weight and height were computed using a 1-way analysis of variance (ANOVA). As alcohol intake (g/d) and the number of cigarettes smoked per day were found to be non-normally distributed, we calculated medians and uesd a Kruskall–Wallis test to evaluate statistical differences between groups.
MRI data acquisition
Magnetic resonance images were obtained with a Magnetom Vision scanner (Siemens) operating at 1.5 T. We scanned all participants with a T1-weighted 3-dimensional magnetization-prepared rapid gradient echo (MPRAGE) sequence (repetition time 11.6 ms, echo time 4.9 ms, total acquisition time 9 min, number of acquisitions 1, field of view 230 mm, matrix 512 × 512, section thickness 1.5 mm) yielding 126 contiguous axial slices with a defined voxel size of 0.45 × 0.45 × 1.5 mm. After manually reorienting and centering the images on the anterior commissure, data were preprocessed using the VBM approach previously shown by Good and colleagues,19 implemented in the VBM5 toolbox (http://dbm.neuro.unijena.de), an extension of the SPM5 software package (Wellcome Trust Centre for Neuroimaging) running under MATLAB 2008b (MathWorks). The VBM 5 toolbox provides state-of-the-art longitudinal VBM preprocessing algorithms. We performed a voxel-based morphometry analysis including DARTEL processing on acquired data.
VBM preprocessing
The present study employed the VBM5 toolbox, which utilizes and extends the new unified segmentation approach implemented in SPM5.20 Unified segmentation provides a generative model of VBM preprocessing that integrates tissue classification, image registration and MRI inhomogeneous bias correction. Thus, the model avoids the “circularity problem” of the optimized VBM procedure, as the initial image registration does not require an initial tissue segmentation or vice versa.19 The VBM5 toolbox extends the unified segmentation model as it increases the quality of segmentation by applying a Hidden Markov Field (HMRF) model on the segmented tissue maps.21 The HMRF algorithm provides spatial constraints based on neighbouring voxel intensities within a 3 × 3 × 3 voxel cube. It removes isolated voxels that are unlikely to be a member of a certain tissue class and also closes holes in a cluster of connected voxels of a certain class, resulting in a higher signal-to-noise ratio of the final tissue probability maps. The VBM5 toolbox also offers the possibility to write the estimated tissue probability maps without making use of the respective International Consortium for Brain Mapping tissue priors from SPM5.
We used this option as it improved the delineation of the subcortical structures and sulci in the final tissue maps. We modulated the final tissue maps of grey matter, white matter and cerebrospinal fluid (CSF) with the deformation fields obtained by normalization to standard space to analyze volume differences between study populations using DARTEL, a suite of tools that allows a highly accurate intersubject registration of brain images. Therefore, grey and white matter images were imported into DARTEL, and nonlinear deformations for their optimal alignment were estimated by alternating between building a template and registering the tissue class images with the template. Subsequently, the Jacobian scaled (“modulated”) warped tissue class images were created. Finally, the grey and white matter partitions were smoothed with an 8-mm full-width at half-maximum Gaussian kernel and used for statistical analysis. We performed an analysis of covariance (ANCOVA) to investigate focal grey and white matter volume differences between participant groups using age and sex as covariates. We defined ROIs16 to test grey and white matter volume differences in the hippocampus, ACC, basal ganglia, DLPFC and DMPFC. We identified ROIs using the Wake Forest University PickAtlas Toolbox, Version 2.0. The PickAtlas software toolbox22,23 provides a method for generating ROI masks based on the Talairach Daemon database.24,25 For the a priori set ROIs, a threshold of p < 0.005 (uncorrected) with a spatial extent threshold of 25 contiguous voxels for group interactions was chosen. To further protect against type-I error, we applied a small volume correction by centering a sphere of 10 mm on the peak voxel (cut-off value: 0.05, family wise error [FWE]–corrected). Additionally, to test for differences in other brain regions, we assessed volume differences (increases/decreases) at the whole-brain level using voxel statistics corrected with FWE (p < 0.05). We assigned coordinates of peak significant voxels to anatomic regions by means of automated anatomic labelling.16,26
Results
Demographic data
Demographic and clinical characteristics of participants are summarized in (Table 1). There were 33 healthy volunteers in the HC-FHP group, 66 in the HC-FHN group and 33 patients with MDD included in this study. Of the patients with MDD, 17 had a positive family history and 16 had a negative family history of MDD. After a careful check of data quality, we excluded 2 participants from the HC-FHN group and 3 from the HC-FHP group because of movement artifacts or incomplete brain scans. No participant had ever received electroconvulsive therapy before investigation. Ten patients with MDD received serotonin reuptake inhibitors (SSRIs), 10 tricyclic antidepressants, 4 venlafaxine, 1 mirtazapine and 2 reboxetine at the time of scanning. Six patients had not yet started an anti-depressant at this time because they came without medication to their admission and were scanned soon after admission. There was no significant difference across groups in age, sex, height, weight, handedness and alcohol daily consumption.
Demographic and clinical characteristics of healthy controls with and without a family history of MDD and patients with MDD
Grey matter volume
With respect to our a priori hypothesis, the ROI analysis (Table 2) revealed a group interaction in 2 regions of the left hippocampus. Also, there was a trend toward significance in the right hippocampus and right caudate nucleus (Fig. 1). The HC-FHP group had smaller volumes than the HC-FHN group in the right hippocampus and right DLPFC (Fig. 2). We found no significantly smaller volumes in the HC-FHN group compared with the HC-FHP group. Further, volumes in the left DMPFC, left ACC and left and right caudate nuclei were smaller in patients with MDD compared with the HC-FHN group. The HC-FHP group also had smaller volumes than the MDD group in the right hippocampus. Patients with MDD also had smaller volumes in the right ACC and right DMPFC compared with the HC-FHP group.
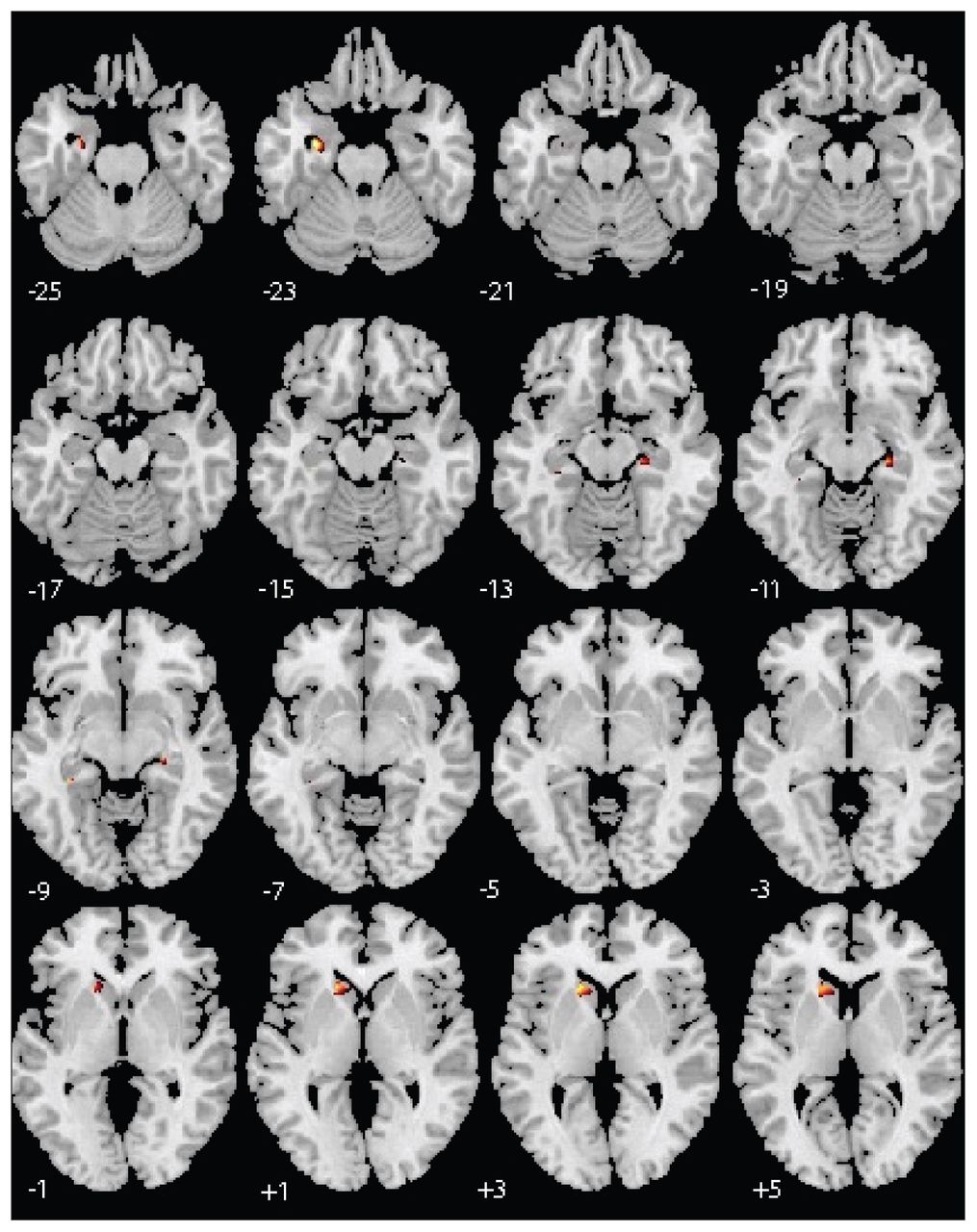
Group interaction. Grey matter differences were found in 2 areas of the left hippocampus (p < 0.05, family wise error– and small-volume corrected).

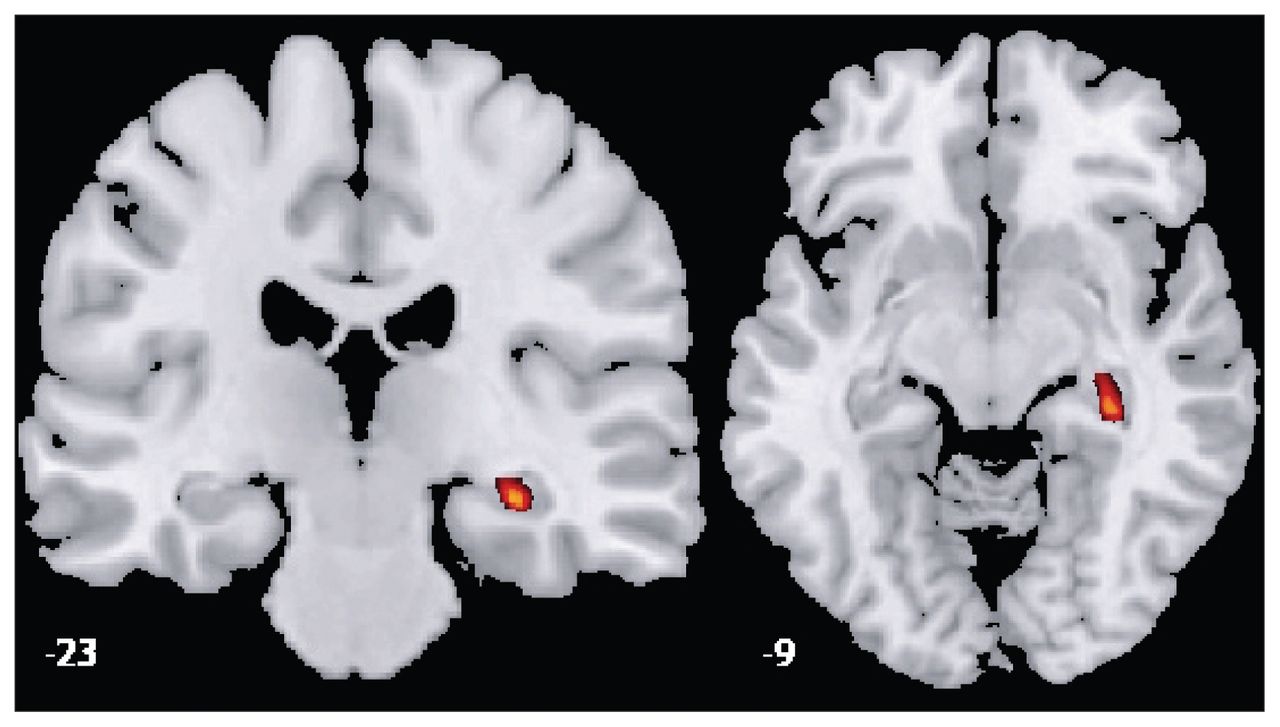
Region of interest grey matter volume comparison between groups of healthy controls with (HC-FHP) and without (HC-FHN) a family history of depression. The HC-FHP group showed smaller volumes in the right hippocampus and right dorsolateral prefrontal cortex (p < 0.05, family wise error– and small-volume corrected).
Comparisons of region of interest grey matter volume between healthy controls with and without a family history of MDD and patients with MDD
At the whole-brain level, the HC-FHP group had smaller volumes in the right medial temporal lobe when compared with the MDD group (p = 0.047, FWE voxel level–corrected; κ = 1238; t = 4.88; x = 66, y = −25, z = −7).
White matter volume
The ROI analysis (Table 3) showed significant group interactions in the right caudate nucleus, left DLPFC and left hippocampus. We detected smaller volumes in the left DLPFC and left putamen in the HC-FHP group compared with the HC-FHN group. The HC-FHP group also had larger volumes in 2 areas of the right DMPFC compared with the HC-FHN group. There was no significant difference between the HC-FHN and MDD groups. Patients with MDD had smaller white matter volumes in the right ACC and right DLPFC compared with the HC-FHP group.
Comparisons of region of interest white matter volume between healthy controls with and without a family history of MDD and patients with MDD
At the whole-brain level, there was a group interaction in areas of the right caudate nucleus (p = 0.046, FWE voxel level–corrected; κ = 254; t = 4.77; x = 19, y = 22, z = −9), but no further effect for differences between subgroups.
Patients with a family history of MDD and those without did not differ with respect to age or sex. Age of onset was earlier as expected in patients with a family history (t1,31 = 2.4, p = 0.02). An exploratory analysis of the differences between patients with and without a family history of MDD did not result in significant differences between groups at the whole-brain level. A comparison between the MDD-FHP and HC-FHP groups revealed smaller right medial temporal cortex volumes in the MDD-FHP group (p = 0.001, FWE voxel–level corrected; κ = 4164; t = 6.04; x = 66, y = −24, z = −8). Keeping in mind our main research question, and given the small samples in these groups, we did not apply an ROI procedure to this comparison to investigate further differences.
Discussion
In the present study, we could partly confirm our primary hypothesis. Participants at greater risk for depression (HC-FHP) had smaller right hippocampal volumes compared with participants at low risk (HC-FHN). These results suggest that reduced hippocampal volumes may be a correlate for increased genetic vulnerability to become depressed, in line with recent evidence showing that, compared with individuals at low familial risk for depression, high-risk individuals exposed to stressful life events have reduced hippocampal volumes independent from the manifestation of clinical symptoms of MDD27,28 and lower blood concentration of brain-derived neurotrophic factor (BDNF),29 a neurotrophin that is expressed abundantly in adult limbic structures. The “BDNF hypothesis” finds support in preclinical literature showing that stress reduces BDNF-mediated signalling in the hippocampus, an effect that is alleviated by chronic treatment with antidepressants.30,31 The present findings might also agree with earlier research showing that patients with MDD who have reduced hippocampal volumes have worse clinical outcomes with more relapses and a more chronic course of the disease.32–34 Interestingly, the changes in the hippocampus were detected only in the right hemisphere. Previous research has consistently shown bilateral hippocampal volume reductions in individuals with a family history of MDD and also suggested that stress might substantially enhance hippocampal morphologic abnormalities in participants at high risk for depression28,35 and in participants carrying the short (risk) allele of the serotonin transporter polymorphism.35 Childhood neglect was associated with left hippocampal volume decreases in a sample of depressed patients.36 Therefore, it is unclear why volume differences reached significance only in the right hippocampus. Remarkable is that we found a significant interaction between family history (yes/no) and depression (yes/no) in the left hippocampus and a trend in the right hippocampus, demonstrating that there were bilateral effects. Further VBM research should confirm this speculation comparing high-risk individuals with and without history of early-life stressful events.
Patients with MDD had smaller grey matter volume in the DMPFC, ACC and caudate nuclei compared with the HC-FHN group, in line with previous studies.37–39 The VBM analysis did not detect smaller hippocampal volumes in patients with MDD as previously shown,33,40 which might be related to technical limitations of the procedure itself, in which voxel-wise statistics about group differences could be biased by registration failure in systematic ways.41 Interestingly, volumetric reductions in the hippocampus, amygdala, ACC and striatum found in depressed participants may be linked to the dysregulation of the “cortico–striatal–pallidal–thalamic” (CSPT) loop activity in depression.42–47 The CSPT is a circuit that includes the PFC and regulates reward-seeking behaviours as well as anticipation and evaluation of rewarding stimuli.48,49 Given that anhedonia is a key symptom in depression, the reduced grey matter volumes we found in both the HC-FHP group and patients with MDD might further strengthen the relation between CSPT dysfunctions and vulnerability to depression. In particular, the grey matter volume reductions found in our HC-FHP participants might also suggest that in high-risk individuals structural remodelling might take place in the hippocampus independently from the onset of MDD symptoms.
Patients with MDD also had smaller grey matter volumes in the right ACC and right DMPFC compared with the HC-FHP group. Moreover, patients with a family history showed further volume decline compared with the HC-FHP group, in line with our previous longitudinal study that showed greater volume decline in the hippocampus and frontal cortices, in particular in those patients with MDD who were not remitted over a 3-year follow-up period.12
To our knowledge, the present study investigated for the first time putative volumetric differences between healthy individuals with and without a family history of depression and patients with MDD. Interestingly, an area in the right hippocampus also was found to be larger in patients with MDD than the HC-FHP group. It should be pointed out that treatment in patients might have a larger influence than pre-viously thought, perhaps inducing volumetric increases in some of the brain structures where significant differences were found, in line with animal studies50 and some pilot studies in humans.33,51 An increase of grey matter volume was detected after a 6-week trial with duloxetine in 15 patients with depression and anxiety compared with the pretreatment unmedicated situation.52
With respect to white matter, patients with MDD had smaller volumes in the right ACC and right DLPFC compared with the HC-FHP group but no differences compared with the HC-FHN group. It is not astonishing that we did not find changes in the hippocampal white matter because this is only a small proportion of the hippocampus and it is impossible to show any significant volume difference in VBM. Moreover, we found smaller left putamen and DLPFC volumes, in line with the hypothesis mentioned above that these structures are involved in the brain network of patients with MDD. However, we also found larger right DMPFC volumes in the HC-FHP compared with the HC-FHN group. One could expect that high-risk participants who did not become depressed, while more likely to carry a high genetic risk, may have some protective neurobiological characteristics. Speculatively, larger DMPFC volumes may be a structural correlate of protective factors, indicating that the HC-FHP participants have a genetic vulnerability and an associated smaller hippocampal volume but also some resiliency factors. New research on resilience showed that induction of the transcription factor DeltaFosB in response to chronic defeat stress is necessary and sufficient for resilience in mice.53 The medial prefrontal cortex is thought to play a role in the top–down regulation of subcortical regions like the amygdala, which has been found to be overactive in patients with MDD.54 In a functional MRI study, high-risk participants had normal functional brain activities when they used their mPFC to constrain their attention.55 An association between resilience to stress and brain structures might also be suggested from a recent study in children with posttraumatic stress disorder showing that a history of stressful life events is associated with greater prefrontal grey matter volume in participants with abnormal emotional regulation and by the evidence suggesting that neurotrophic factors themselves do not control mood, but might influence networks whose physiologic functions determine how plastic changes influence mood.56 Moreover, our findings agree with a recent animal study in which Rhesus monkeys were divided into 2 groups at birth: a group raised by their mothers and other juvenile/adult animals and a group raised by 3 age-matched monkeys only for the first 6 months of life. Magnetic resonance imaging revealed that the DMPFC, dorsal ACC and vermis were enlarged in the animals raised only by the age-matched monkeys, suggesting that an enlargement of stress-sensitive brain regions could be a phenotype of psychiatric disorders.57
However, the hypotheses that MDD and family history of depression could be associated with white matter volume increases and that these larger brain volumes may even have protective effects against the development of MDD should be confirmed by well targeted longitudinal studies, and the neurobiological background of volume increase needs to be examined.
Limitations
Limitations of the present study might derive from the methodology we used to assess family history of depression. Asking participants about psychiatric history and diagnosis of their family members results in moderate sensitivity also in structured interviews, thus increasing the probability for screening errors.58 Intelligence has been shown to be significantly associated with aberrant myelination and synaptogenesis in the brain.59,60 Therefore, future investigations should also control for intelligence.
Finally, our patient sample size was too small to demonstrate definitive differences in patients with and without a family history of MDD. Our primary aim was to show differences between HC-FHP and HC-FHN participants and to compare them with patients with MDD. An exploratory analysis between patients with MDD with and without family history of depression did not show differences as expected because of sample size. These results also show that sample sizes of 30 or more participants may be a prerequisite for automatic structural brain imaging analysis, and smaller groups should not be treated with ROI procedures.
Conclusion
The present study suggests that reduced grey matter volume in the hippocampus and PFC are associated with a higher risk for MDD. In line with previous evidence, depressed patients exhibited reduced grey matter volume in the PFC, ACC and basal ganglia. Interestingly, larger volumes, particularly white matter, were detected in healthy participants and patients with a family history of depression. To what extent these larger volumes are associated with resilience to stress or depressive vulnerability needs to be investigated in further studies.
Acknowledgement
This study was supported from a Research Grant from the Friedrich-Baur-Institute Munich.
Footnotes
Competing interests: None declared for Drs. Amico, Meisenzahl, Koutsouleris, Reiser and Frodl. Dr. Möller declares having received grants from or sitting on the speaker bureaus of AstraZeneca, Bristol-Myers Squibb, Eisay, Eli Lilly, GlaxoSmithKline, Janssen, Cilag, Lundbeck, Merck, Novartis, Organon, Pfizer, Sanofi-Aventis, Schering-Plough, Schwabe, Sepracot, Servier and Wyeth.
Contributors: Drs. Meisenzahl, Reiser and Frodl designed the study. Drs. Koutsouleris and Frodl acquired the data, which Drs. Amico, Meisenzahl, Koutsouleris, Möller and Frodl analyzed. Drs. Amico, Meisenzahl and Frodl wrote the article, which Drs. Meisenzahl, Koutsouleris, Reiser, Möller and Frodl reviewed. All authors approved the article’s publication.
- Received December 31, 2009.
- Revision received May 4, 2010.
- Revision received June 8, 2010.
- Accepted June 11, 2010.
References
In this issue

{kind=link}
{kind=link}
Article tools





