

Article Figures & Tables
Figures
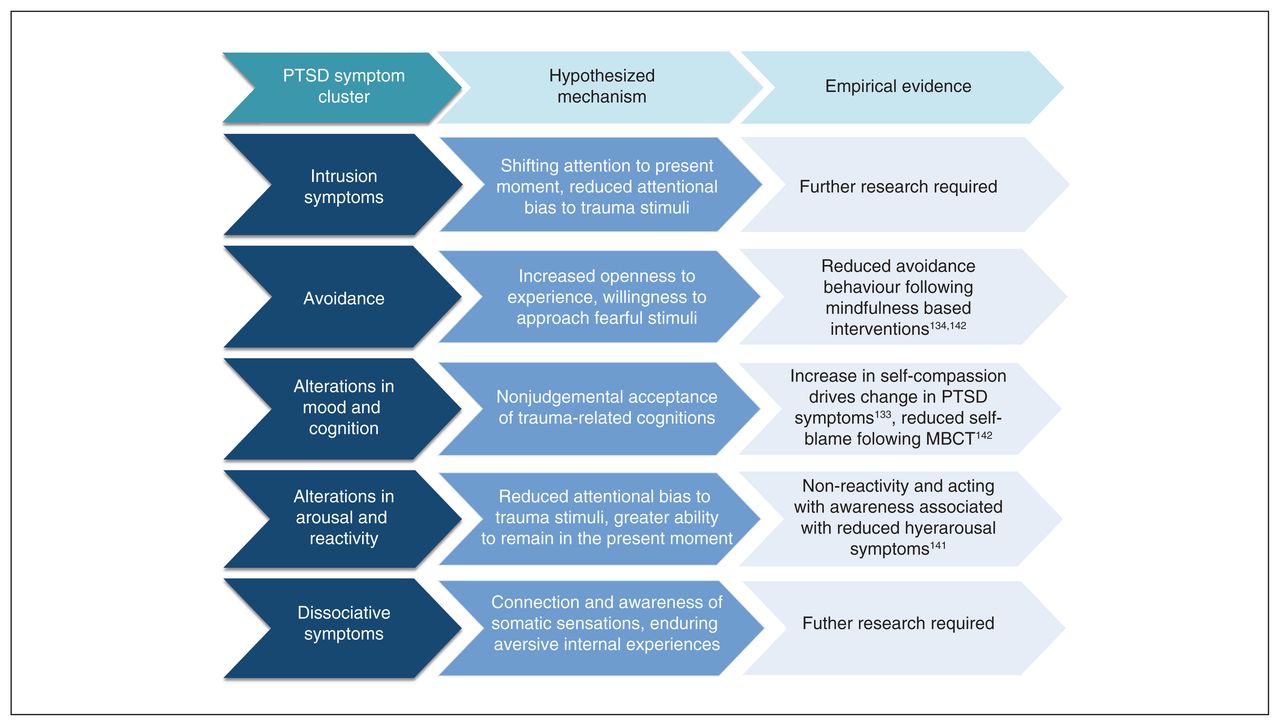
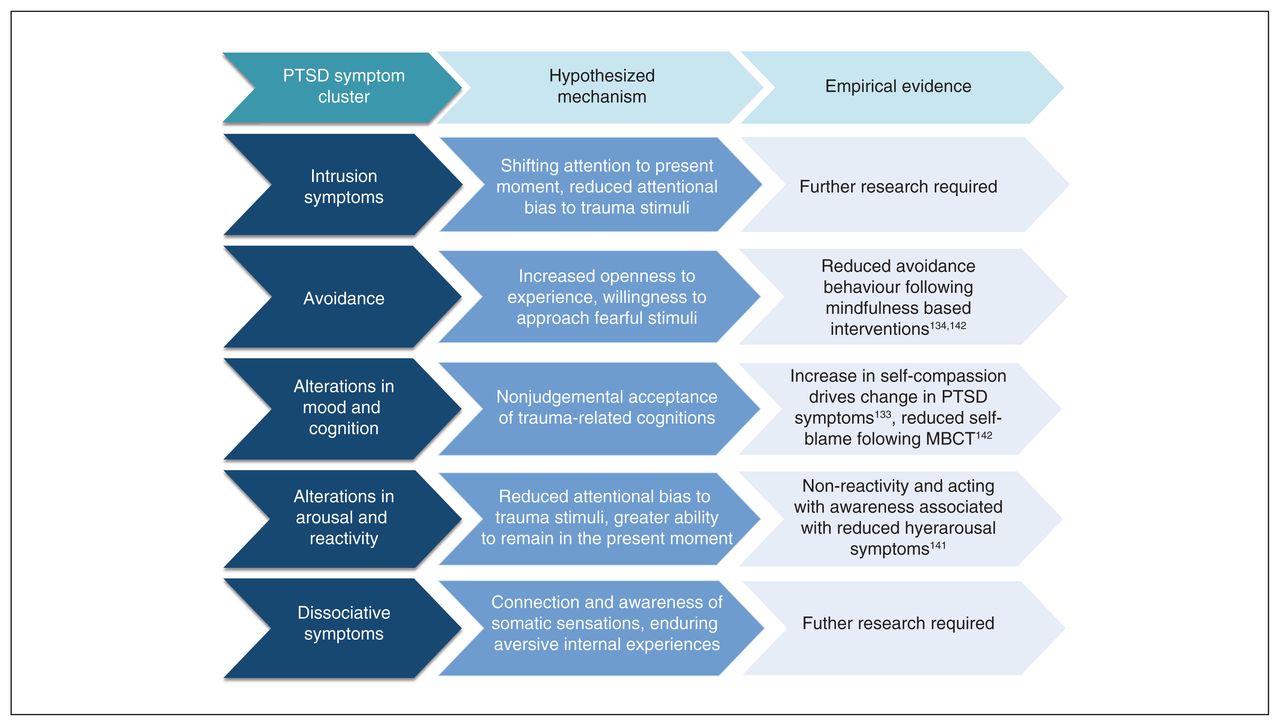
- Fig. 1
Hypothesized mechanisms by which mindfulness-based approaches may target posttraumatic stress disorder (PTSD) symptom clusters along with current evidence and indication of where further research is required. MBCT = mindfulness-based cognitive therapy.
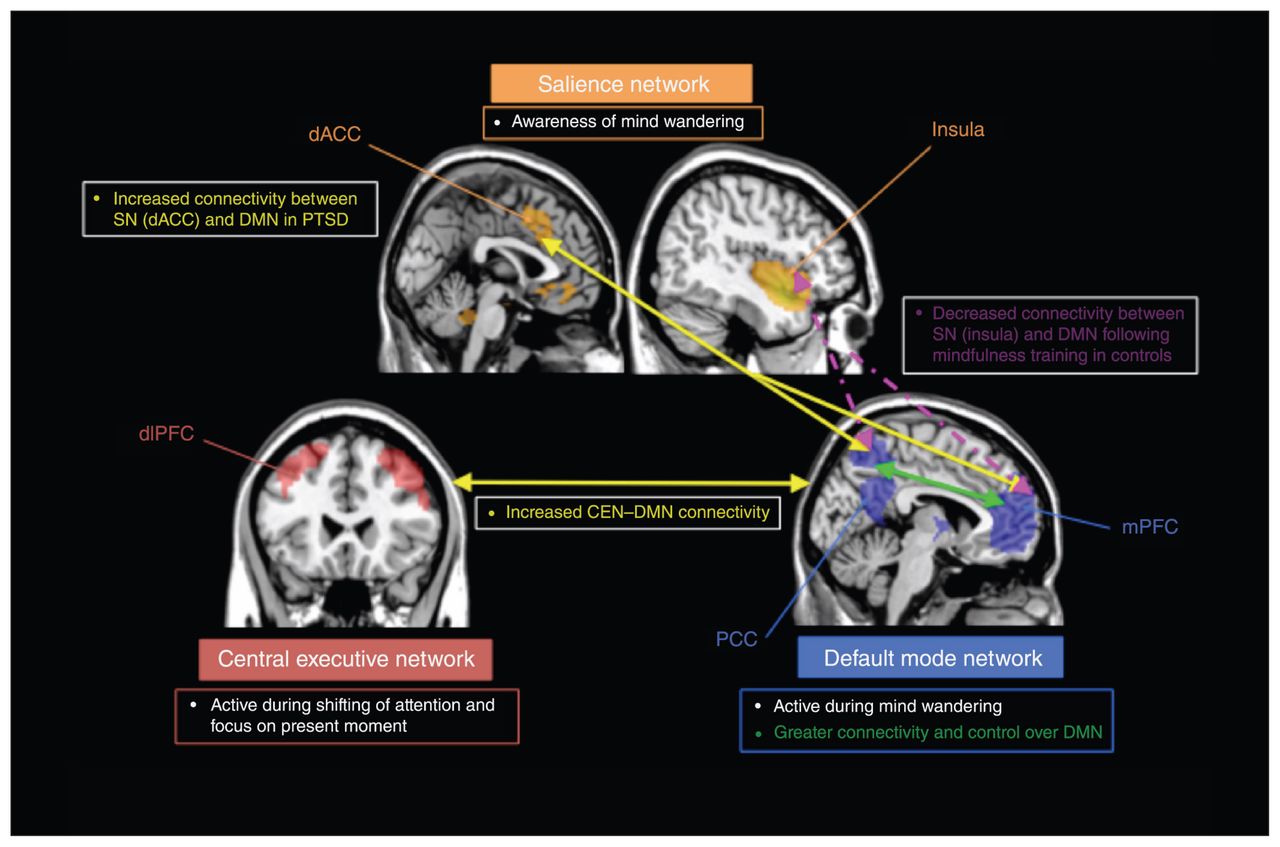
- Fig. 2
Summary of the current literature implicating alterations in functional connectivity within and between the salience network (SN; shown in orange), the central executive network (CEN; shown in red) and the default mode network (DMN; shown in blue) in individuals with posttraumatic stress disorder (PTSD). Reduced connectivity within networks is depicted by red dashed lines, increased connectivity within networks is depicted by solid green lines, reduced connectivity between networks is depicted by pink dashed lines, and increased connectivity between networks is depicted by solid yellow lines. Consistent findings indicate reduced functional connectivity within the DMN among those with PTSD, posited to underlie disruptions in self-referential processes, autobiographical memory and altered sense of self. Conversely, increased connectivity is reported within the SN, thought to underlie hyperarousal and increased threat sensitivity. Similarly, increased connectivity between the DMN and SN is thought to reflect hypersensitivity to threat at the expense of self-referential processing. Individuals with PTSD also show impaired ability to appropriately recruit relevant networks (e.g., activation of DMN rather than CEN during a working memory task), suggesting impaired switching between the DMN and CEN via the SN. Distinct patterns of connectivity within the CEN have emerged among those with PTSD and PTSD with dissociative symptoms (PTSD+DS); those with PTSD+DS showed increased connectivity within the CEN and those with PTSD showed decreased connectivity within the CEN. dACC = dorsal anterior cingulate cortex; dlPFC = dorsolateral prefrontal cortex; mPFC = medial prefrontal cortex; PCC = posterior cingulate cortex.
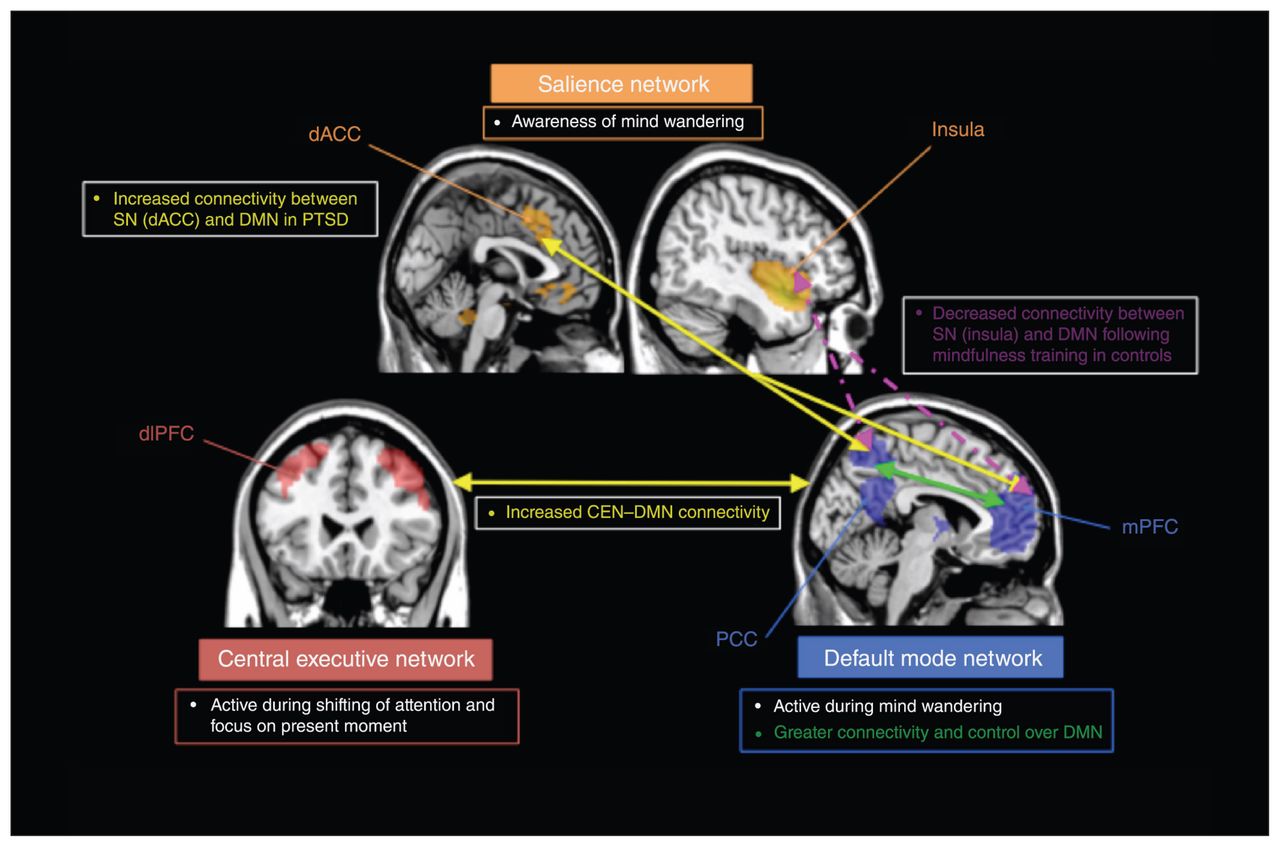
- Fig. 3
Summary of findings suggesting that mindfulness may lead to restoration of functioning of the salience network (SN; shown in orange), central executive network (CEN; shown in red) and defult mode network (DMN; shown in blue). Increased connectivity within networks is depicted by solid green lines, increased connectivity between networks is depicted by solid yellow lines, and reduced connectivity between networks is depicted by dashed pink lines. Emerging work has indicated greater functional connectivity within the DMN during rest among meditators when compared with controls and among veterans with posttraumatic stress disorder (PTSD) following mindfulness intervention, suggesting that it may restore DMN connectivity and appropriate self-referential processing in those with PTSD. (35) Increased CEN–DMN connectivity was also reported and may reflect increased ability to shift between internal and external loci of attention. Mixed findings of both increased and decreased DMN–SN connectivity following mindfulness intervention have been reported, depending on the region of the SN. Increased dorsal anterior cingulate cortex (dACC)–DMN connectivity was reported following mindfulness intervention for PTSD, (35) which may suggest increased capacity for attentional shifting from internal to external stimuli (dACC implicated in executive control). In contrast, reduced SN (insula)–DMN connectivity was reported among controls, which may result in reduced hyperarousal symptoms and increased self-referential processing if findings were replicated in individuals with PTSD. dlPFC = dorsolateral prefrontal cortex; mPFC = medial prefrontal cortex; PCC = posterior cingulate cortex.

Tables
Study Sample Assigned therapy Assessments Study type Attrition Main findings Bergen-Cico et al. (135) 40 veterans (90% male) with PTSD BMP based on MBSR (4 weekly 90-min sessions) plus TAU or to TAU alone (typical primary care for veterans) Salivary cortisol PCL, PHQ-9 (measure of depression) RCT, pre/post measures 20% drop-out rate BMP completers showed significant reduction in CAR (0.2 μg/dL)
TAU and noncompleters did not show a significant decrease in CAR
Significant correlation between changes in cortisol levels and PTSD and depression scoresBormann et al. (146) 146 veterans (142 male) with PTSD MRP (6 weekly 90-min classes) or TAU alone (case management and consultation as needed) CAPS, PCL-C, BSI-18 (depressive symptom subscale), SF-12 (mental health component), MAAS RCT, pre/post measures 95% of MRP+TAU completed treatment Significantly greater reduction in PCL-C, CAPS hyperarousal and numbing symptoms, depression, and mental HRQOL in MRP+TAU group
Significantly greater improvement on MAAS in MRP+TAU group
Mindful attention mediated effect of MRP on PTSD, depression and psychological well-being measures
Daily mantrum practice mediated effect of MRP on mindful attentionCatani et al. (145) 31 children (17 male) exposed to tsunami with working diagnosis of PTSD Meditation–relaxation (individual psychoeducation and meditation relaxation strategies) or KIDNET (individual narrative exposure therapy adapted for children) UPID (5 items to assess problems in functioning, 5 items to assess presence of somatic complaints) RCT, pre/post measures; 6-mo follow-up 100% completed full treatment No significant difference between groups on PTSD symptoms
Significant reduction in PTSD scores within meditation–relaxation group immediately posttreatment (d = 1.83) and at follow-up (d = 2.20)
71% of meditation–relaxation children did not meet criteria for PTSD at 6-mo follow-up and 81% did not meet criteria in KIDNET group (no significant difference)
Significant improvement on functional scores in both treatment groups (no significant difference)Cole et al. (129) 10 veterans with history of mTBI and PTSD MBSR (1 introductory 2-hr class, 8 weekly 2.5-hr sessions, 1 7-hr retreat) PCL-C, Cogstate computerized assessment to measure attention Single arm, uncontrolled study, pre/post measures; 3-mo follow-up 90% completed treatment Significant reductions in PCL-C scores immediately posttreatment (d = 1.56) and at follow-up (d = 0.93)
Significant improvement on attention measures immediately posttreatment (d = 0.57), not maintained at follow-upEarley et al. (130) 19 women survivors of CSA with general severity index BSI score > 0.50 MBSR (8 weekly 2.5–4 hr classes and 1 5-hr retreat (augmented for CSA) with concurrent psychotherapy BDI-II, PCL, BSI-18, MAAS Single arm, uncontrolled study; 2.5-yr follow-up of previous study (133) NA Improvements at 1 mo posttreatment maintained at 2.5-yr follow-up for depression (d = 1.10), anxiety (d = 0.90), and PTSD symptoms (d = 0.80)
PCL subscales significantly lower from baseline at 2.5-yr follow-up: avoidance/numbing (d = 0.70), re-experiencing (d = 0.50), hyperarousal (d = 0.90)Gallegos et al. (139) 42 women with history of interpersonal violence and high perceived stress MBSR (8 weekly 2.5-hr sessions, 1 day-long retreat) TLEQ, STAI, DERS, CDES, MPSS, FFMQ, IL-6, TNF-α, CRP Single arm, uncontrolled study, pre/mid/post measures; 1-mo follow-up 57% completed more than 50% of classes Significant reductions in depressive symptoms at all time points
Significant reductions in PTSD symptoms, state and trait anxiety immediately posttreatment and at follow-up
Significant improvement in DERS scores immediately posttreatment and at follow-up
Significant effect of attendance on IL-6 levels (reduced IL-6 with increased attendance)Goldsmith et al. (131) 10 individuals with exposure to lifetime trauma or childhood abuse (9 female) with primary diagnosis of PTSD or MDD MBSR (8 weekly 2.5-hr sessions with 1 day-long retreat) PHQ-9, BDI-II, PCL, CTQ, LEC, AAQ-II (measure of experiential avoidance), TAQ Single arm, uncontrolled study, pre/mid/post measures 90% retention Significant reduction at mid-treatment and post-treatment in PTSD symptoms (d = 0.70, d = 0.73), depression (d = 0.30, d = 0.54) and TAQ shame-based appraisals (d = 0.30, d = 0.70)
Significant improvement in AAQ scores mid-treatment and post-treatment (d = 0.77, d = 1.11)Kearney et al. (132) 92 veterans with PTSD MBSR (8 weekly 2.5-hr sessions and 1 7-hr retreat) PCL-C, PHQ-9, BADS, SF-8 (mental and physical HRQOL), AAQ-II, FFMQ Single arm uncontrolled study, pre/post measures; 4-mo follow-up 74% met minimum compliance (4 of 8 classes) Significant improvement at baseline and follow-up on PCL total (d = 0.55; d = 0.65), PCL re-experiencing (d = 0.40; d = 0.56), avoidance (d = 0.36; d = 0.35), emotional numbing (d = 0.46; d = 0.54), and hyperarousal (d = 0.64; d = 0.67)
Significant improvement at baseline and follow-up on depression score (PHQ-9; d = 0.53; d = 0.70), BADS (d = 0.47; d = 0.62), mental HRQOL (d = 0.62, d = 0.73), and AAQ (d = 0.65; d = 0.68)
Clinically significant reductions in PCL scores in 47.7% of participants
Changes in FFMQ scores from baseline to post-treatment significantly predicted PCL, PHQ-9, mental HRQOL immediately post-treatment and at follow-upKearney et al. (133) 47 veterans (37 men) with chronic PTSD MBSR (8 weekly 2.5-hr sessions and 1 7-hr retreat) plus TAU or TAU (usual care for PTSD within veterans health administration clinics) PCL-C, LEC, PHQ-9, SF-8, FFMQ, BADS RCT, pre/post measures; 4-mo follow-up 84% met minimum compliance in MBSR group (4 of 8 sessions) No significant difference between MBSR and TAU groups on PTSD, depression or behavioural activation immediately post-intervention or at follow-up
Significantly greater improvement in mental HRQOL in MBSR group post-treatment (d = 0.69), but this was not maintained at follow-up
Significant within-group improvement in the MBSR group on PTSD (d = 0.64), depression (d = 0.65), and mental HRQOL (d = 0.77) post-treatment (maintained only for mental HRQOL at follow-up)
Significant improvement in mindfulness scores immediately post-treatment (d = 0.65) and at follow-up (d = 0.67) in the MBSR groupKing et al. (142) 37 veterans with long-term (> 10 yr) PTSD or PTSD in partial remission MBCT adapted for PTSD (8 weekly 8-hr group sessions) or TAU (psychoeducation and skills training, 8 weekly 1-hr sessions) or imagery research therapy (6 weekly 1.5-hr sessions) CAPS (all groups), PDS (MBSR group only), PTCI (MBSR group only) Nonrandomized controlled study, pre/post measures Dropout 25% in MBCT and 23.4% in TAU groups Significant reduction in CAPS score (d = 2.20) within MBCT group (ITT)
Significantly greater improvement on CAPS score in MBCT than in TAU group (d = 1.14; ITT)
Improvements on CAPS score in MBCT group explained by significant reduction in avoidant subscale (d = 2.11; ITT)
Significant reductions in CAPS intrusive (d = 0.64) and hyperarousal (d = 0.78) symptoms also seen in MBCT group (ITT)
73% in MBCT group attained clinically significant reductions in CAPS score (33% in TAU group; completer analysis)
Significant reduction in PDS numbing subscale (d = 0.57) and PTCI self-blame cognitions (d = 1.80) in MBCT group (completer analysis)King et al. (35) 43 veterans with PTSD MBET (16-wk nontrauma focused intervention; mindfulness, psychoeducation, self-compassion training; in-vivo exposure to avoided situations [no trauma exposure]) or PCGT (16-wk intervention identifying current stressors contributing to PTSD) CAPS RCT, pre/post measures Not reported MBET participants attended an average of 13.5 of 16 sessions; PCGT group attended an average of 7.5 of 16 sessions
No significant differences between groups on PTSD symptom severity differences between pre- and post-treatment assessments
MBET group showed significant reduction in total CAPS (d = 0.96), CAPS intrusion (d = 0.72) and CAPS avoidance (d = 0.97) symptoms
PCGT group showed significant reduction in CAPS hyperarousal symptoms only (d = 0.79)Kim et al. (143) 22 nurses with PTSD, 7 healthy control nurses MBX (16 semi-weekly 60-min sessions) or control condition PCL-C, serum cortisol, plasma ACTH, DHEAS RCT, pre/post measures; 2-mo follow-up Not reported Significantly greater decrease in PTSD symptoms and cortisol levels in MBX group than in controls
No significant differences between groups in ACTH and DHEAS levels
MBX group showed significant reductions in PTSD symptoms (including re-experiencing, avoidance, and hyperarousal) at 2-mo follow-up
Significant association between cortisol levels and PTSD symptomsKimbrough et al. (134) 27 survivors of CSA (24 women) with general severity index BSI score > 0.50 MBSR (8 weekly 2.5–4 hr classes and 1 5-hr retreat augmented for CSA) with concurrent psychotherapy BDI-II, PCL, BSI, MAAS, practice logs and attendance monitoring Single arm uncontrolled study, pre/mid/post measures; 4-mo follow-up 85% retention Significant reduction immediately post-treatment and at follow-up on depression scores (d = 1.8; d = 1.0), anxiety (BSI; d = 1.1; d = 0.90), PTSD symptoms (d = 1.2; d = 1.0)
Significant reductions immediately post-treatment and at follow-up on PTSD avoidance/numbing (d = 1.4; d = 0.90), re-experiencing (d = 0.70 both time points), and hyperarousal (d = 1.2; d = 0.60)
Significant reduction in individuals meeting criteria for PTSD post-treatment but not at follow-upNiles et al. (137) 33 veterans with current PTSD MBSR-based telehealth group (2 45-min in-person sessions and 6 20-min weekly phone calls with weekly individual practice) or telehealth psychoeducation with same contact CAPS, PCL-M, PSQ RCT, pre/post measures; 6-wk follow-up 76% completed MBSR treatment MBSR group showed significant decrease in PCL score (d = 0.84) and decrease in CAPS score (d = 0.70)
At 6-wk follow-up, changes in PTSD in MBSR group were not sustained (d = 0.16)
Significantly greater improvement in MBSR group at posttreatment on PCL (d = 1.95) and CAPS scores (d = 1.27)Polusny et al. (138) 116 veterans with PTSD or subthreshold PTSD MBSR (8 weekly 2.5-hr sessions and 1 day-long retreat) or PCT (9 weekly 1.5-hr sessions) PCL, CAPS, PHQ-9, FFMQ, WHOQOL RCT, pre/post measures; 2-mo follow-up Dropout 22.4% in MBSR and 6.9% in PCT Significantly greater reductions in PCL (d = 0.40), CAPS (d = 0.41), WHOQOL (d = 0.41) scores in MBSR group between baseline and 2-mo follow-up
Nonsignificant differences between groups on depressive scores (similar improvement in both groups)
Improvements of FFMQ scores significantly correlated with PTSD (PCL), depression and WHOQOL scoresPossemato et al. (136) 62 veterans with PTSD or subthreshold PTSD BMP (based on MBSR, 4 weekly 90-min sessions) plus TAU or TAU alone (typical primary care for veterans) CAPS, PCL, PHQ-9, FFMQ, MAAS RCT, pre/post measures; 1-mo follow-up 20% dropout rate No significant difference between BMP+TAU and TAU groups using ITT analysis for CAPS and PCL scores
Significantly greater improvement in BMP+TAU group on depression scores (d = 0.86)
BMP+TAU completers showed significantly larger decreases in PTSD severity (CAPS; d = 0.72) and depression scores (PHQ-9; d = 0.99)
FFMQ describing, nonjudgment and acting with awareness and MAAS scores accounted for 30% of total effect of BMP completion on PTSD severityRosenthal et al. (144) 7 veterans with PTSD (all men) TM (taught in 2 information lectures, brief personal interview, individual instruction and 3 follow-up sessions on 3 consecutive days; participants asked to meditate at home for 20 min twice daily for 12 wk) CAPS, PCL-M, Q-LES-Q, BDI, CGI-S, CGI-I, CES Single arm uncontrolled trial, pre-treatment measures; 8-wk follow-up 71% completed Significant improvement on CAPS, Q-LES-Q, PCL-M, CGI-I at week 8 AAQ-II = Acceptance and Action Questionnaire-II; ACTH = adrenocorticotropic hormone; BADS = Behavioural Activation for Depression Scale; BDI-II = Beck Depression Inventory-II; BMP = Brief Mindfulness Program; BSI-18 = 18-item Brief Symptom Inventory; CAPS = Clinician-Administered PTSD scale; CAR = cortisol-awakening response; CDES = Center for Epidemiological Studies Depression Scale; CES = Combat Exposure Scale; CGI-I = Clinical Global Impression Improvement; CGI-S = Clinical Global Impression Severity; CRP = C-reactive protein; CSA = childhood sexual abuse; CTQ = Childhood Trauma Questionnaire; DERS = Difficulties in Emotion Regulation Scale; DHEAS = dehydroepiandrosterone sulfate; FFMQ = Five Factor Mindfulness Questionnaire; HRQOL = health-related quality of life; IL-6 = interleukin-6; ITT = intention to treat; MAAS = Meditation Attention and Awareness Scale; MBSR = mindfulness-based stress reduction; MBX = mindfulness-based stretching and deep breathing exercises; MDD = major depressive disorder; MPSS = Modified PTSD Symptom Scale; LEC = Life Events Checklist; MBET = mindfulness-based exposure therapy: MRP = mantram repetition practice; mTBI = mild traumatic brain injury; NA = not applicable; PCGT = present-centred group therapy; PCL = PTSD Check List; PCL-C = PTSD Check List–Civilian; PCL-M = PTSD Check List–Military; PDS = PTSD Diagnostic Scale; PHQ-9 = Patient Health Questionnaire-9; PSQ = Patient Satisfaction Questionnaire; PTCI = Post-traumatic cognitions inventory; PTSD = posttraumatic stress disorder; Q-LES-Q = quality of life enjoyment and satisfaction questionnaire; RCT = randomized controlled trial; SF-8/SF-12 = 8-item/12-item Short-Form Health Survey; STAI = Spielberger State-Trait Anxiety Inventory; TAQ = Trauma Appraisals Questionnaire; TAU = treatment as usual; TLEQ = Traumatic Life Events Questionnaire; TM = transcendental meditation; TNF-α; tumour-necrosis factor-α; UPID = University of California, Los Angeles PTSD index for DSM-IV; WHOQOL = World Health Organization Quality of Life.

{kind=link}
{kind=link}
{kind=link}
Article tools





