

Article Figures & Tables
Figures
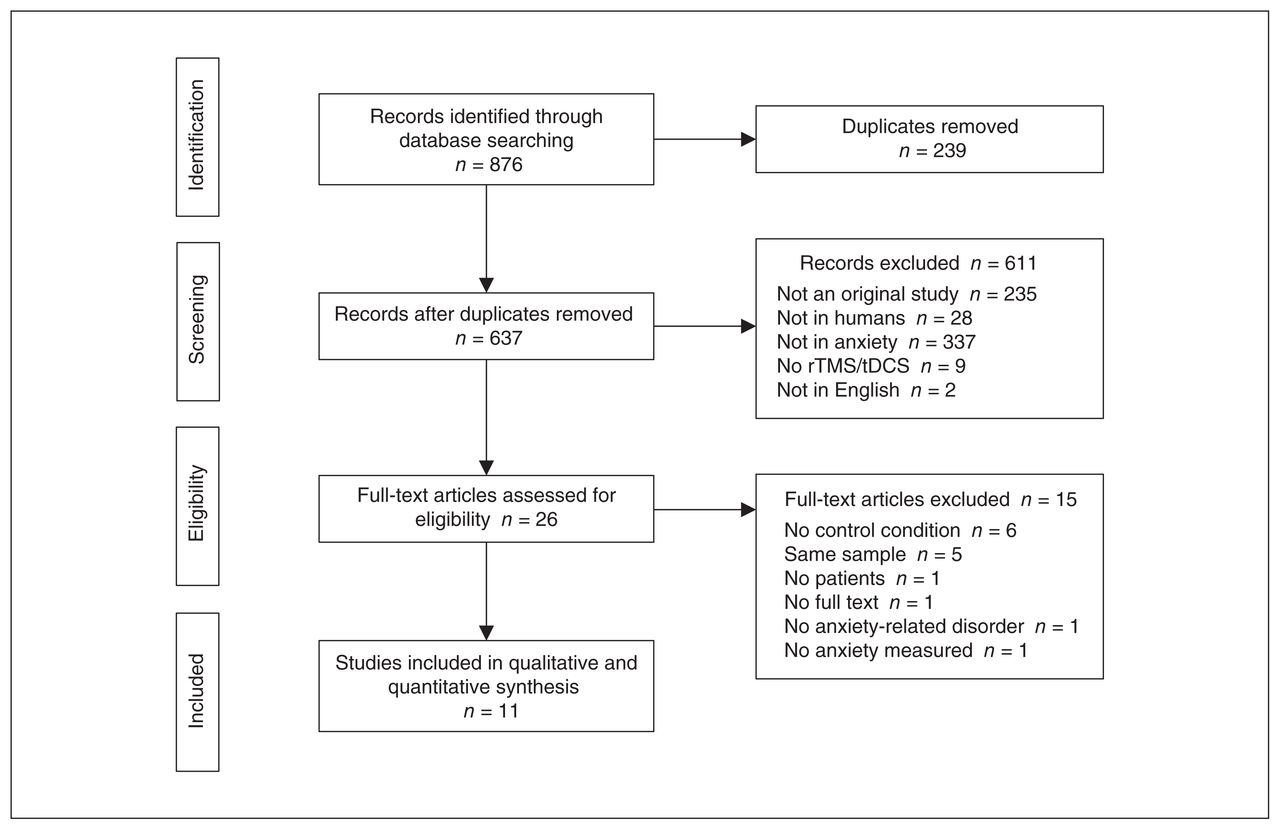
- Figure 1
Flow chart of study selection. rTMS = repetitive transcranial magnetic stimulation; tDCS = transcranial direct current stimulation.
- Figure 2
Type of stimulation and target regions in included studies. Red dots indicate excitatory stimulation protocols (i.e., anodal tDCS, iTBS and high-frequency rTMS); blue dots indicate inhibitory stimulation (i.e., cathodal tDCS and low-frequency rTMS). The size of the dots correspond to the number of studies that applied an excitatory or inhibitory protocol over a specific region: 5 studies applied inhibitory stimulation protocols over the right dorsolateral prefrontal cortex, 3 studies applied excitatory stimulation protocols over the left dorsolateral prefrontal cortex, 1 study applied an excitatory stimulation protocol over the right dorsolateral prefrontal cortex, 1 study applied an inhibitory stimulation protocol over the right posterior parietal cortex, and 1 study applied an excitatory stimulation protocol over the ventromedial prefrontal cortex. Brain images were obtained from www.nitrc.org. iTBS = intermittent theta burst stimulation; rTMS = repetitive transcranial magnetic stimulation; tDCS = transcranial direct current stimulation.
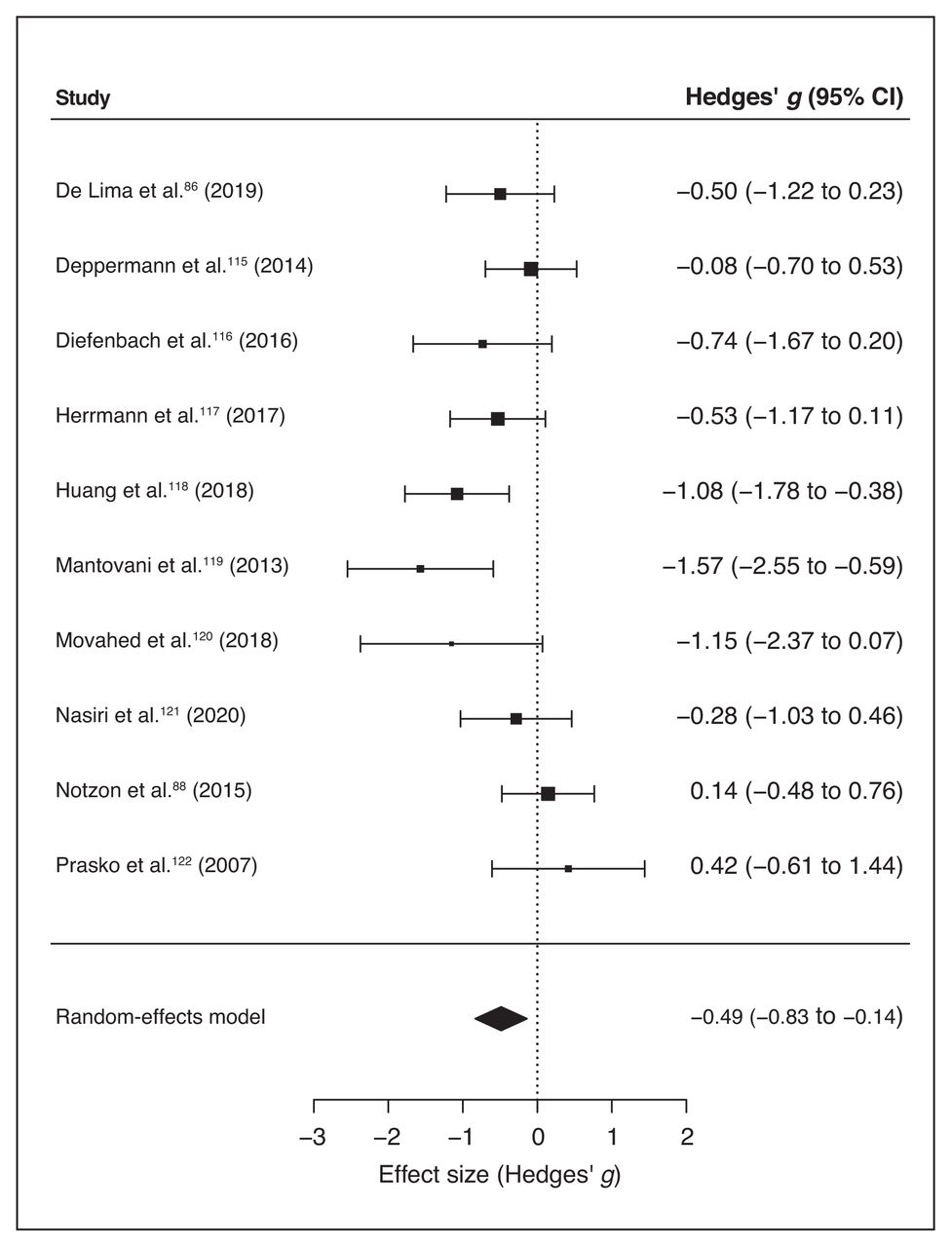
- Figure 3
Forest plot of the effect size of noninvasive brain stimulation on continuous specific anxiety questionnaire scores. CI = confidence interval.
- Figure 4
Baujat plot of study distribution in terms of heterogeneity for continuous specific anxiety questionnaire scores. On visual inspection, study 8 (119) seemed to contribute most to the statistical heterogeneity of the included studies.
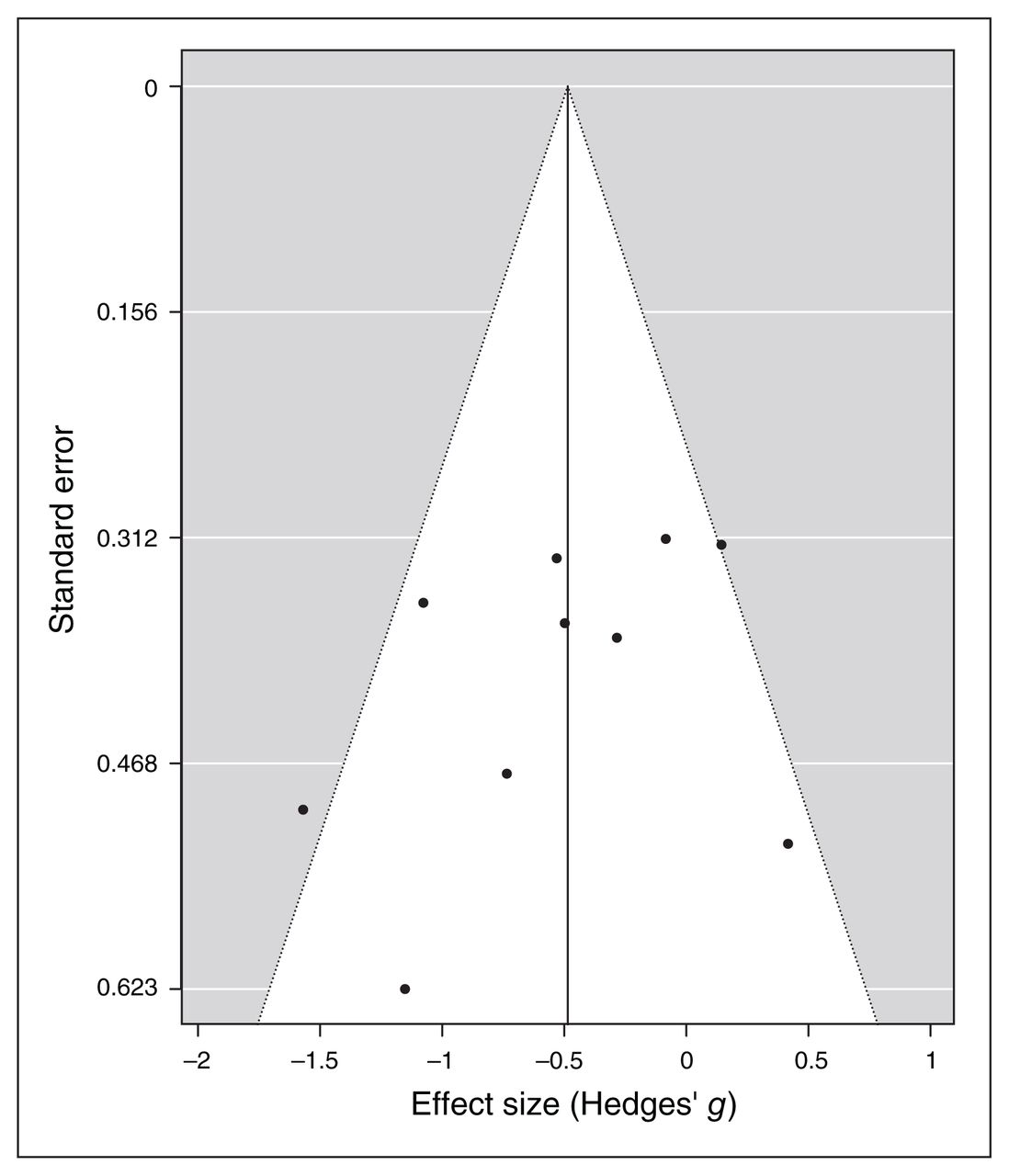
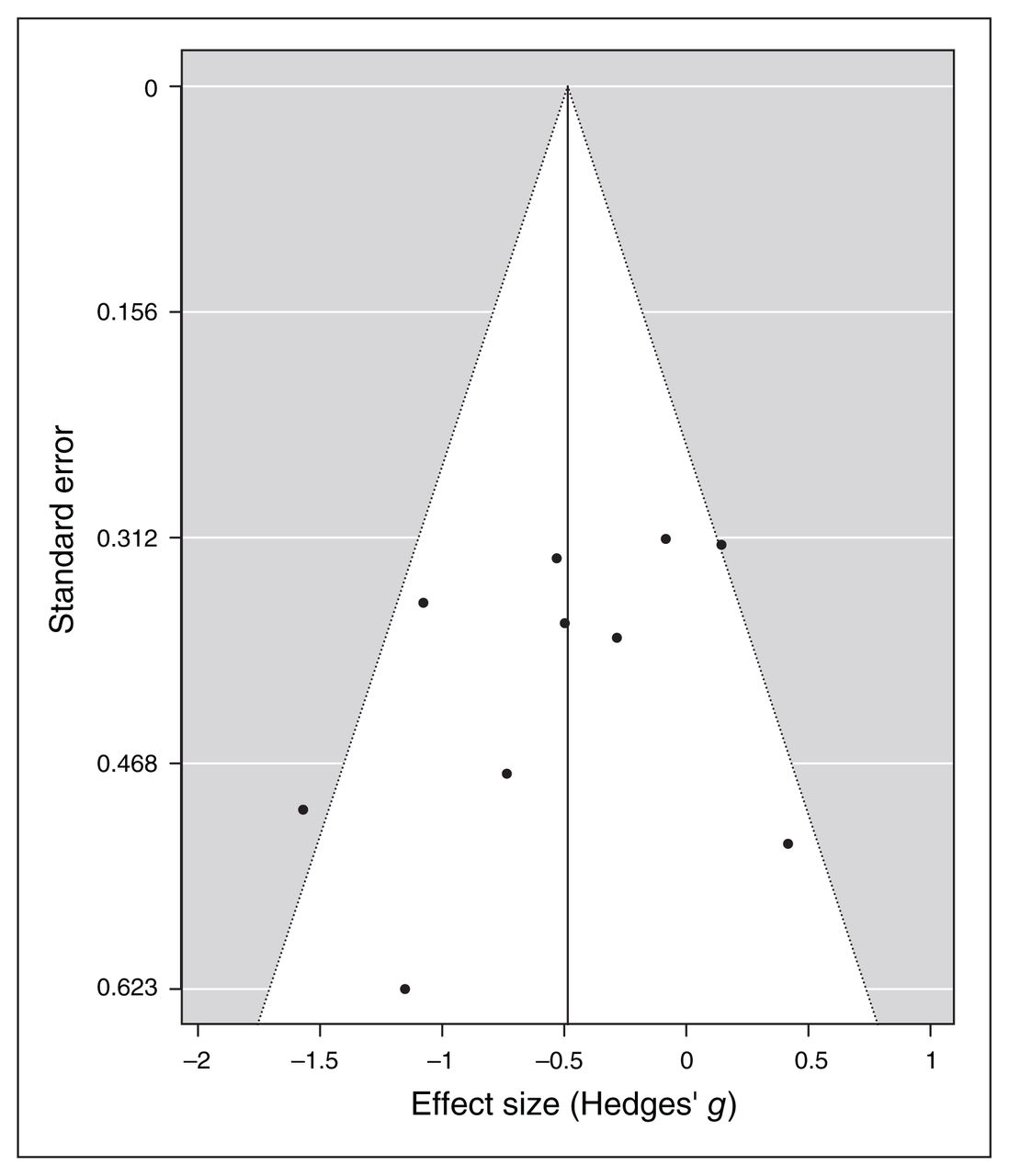
- Figure 5
Publication bias assessed by funnel plot for continuous specific anxiety questionnaire scores.
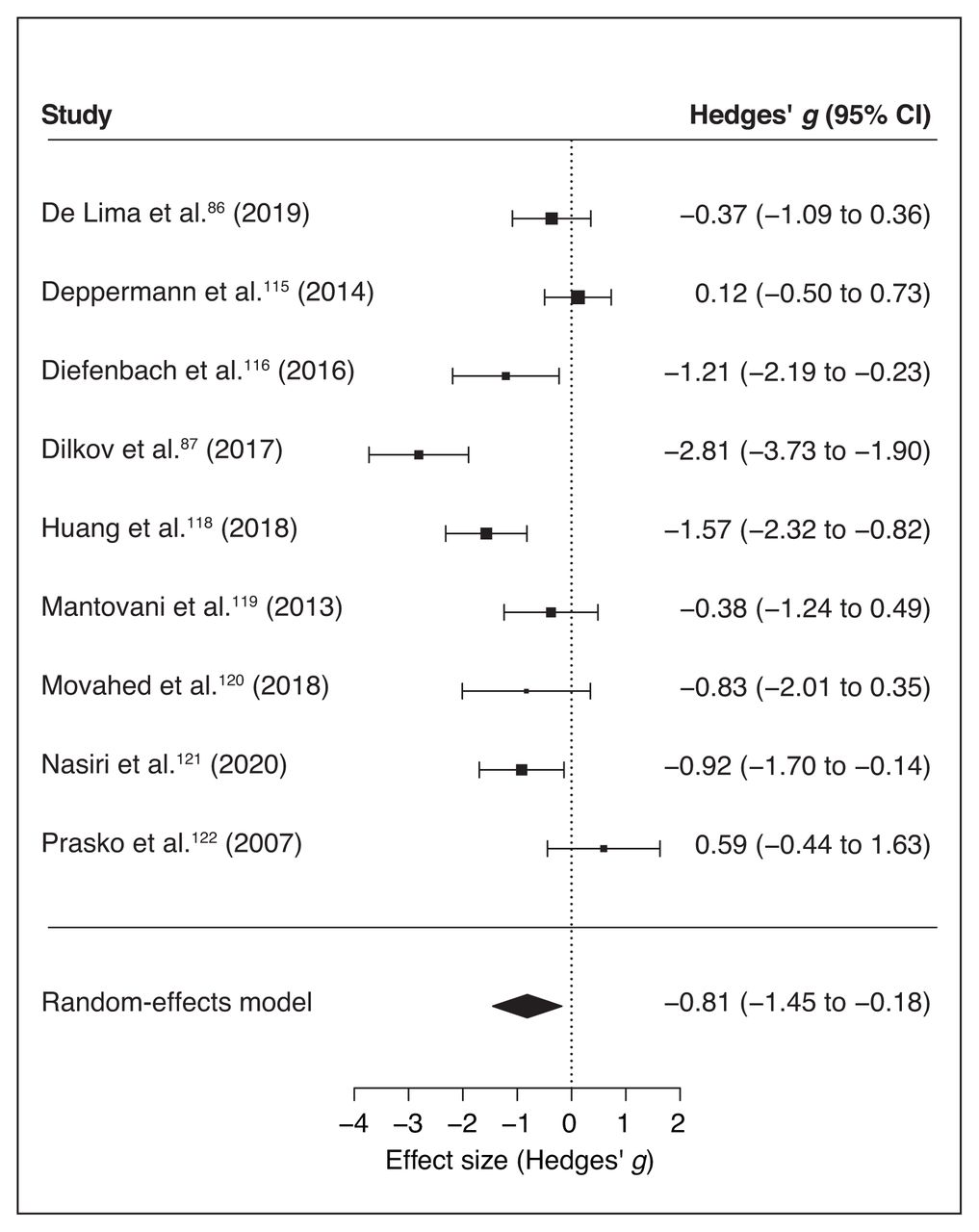
- Figure 6
Forest plot of the effect size of noninvasive brain stimulation on continuous general anxiety questionnaire scores. CI = confidence interval.
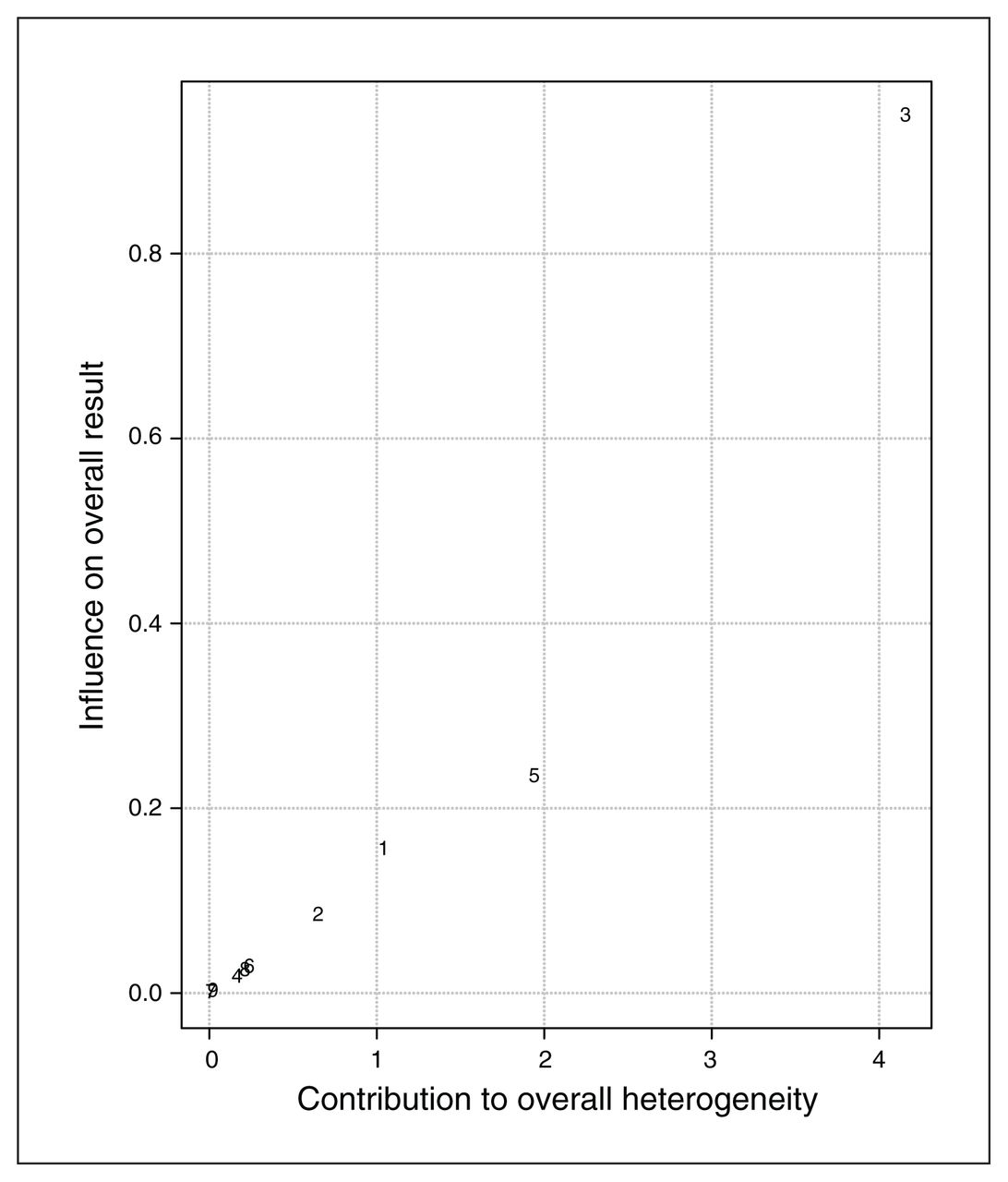
- Figure 7
Baujat plot of study distribution in terms of heterogeneity for continuous general anxiety questionnaire scores. On visual inspection, study 3 (87) seemed to contribute most to the statistical heterogeneity of the included studies.
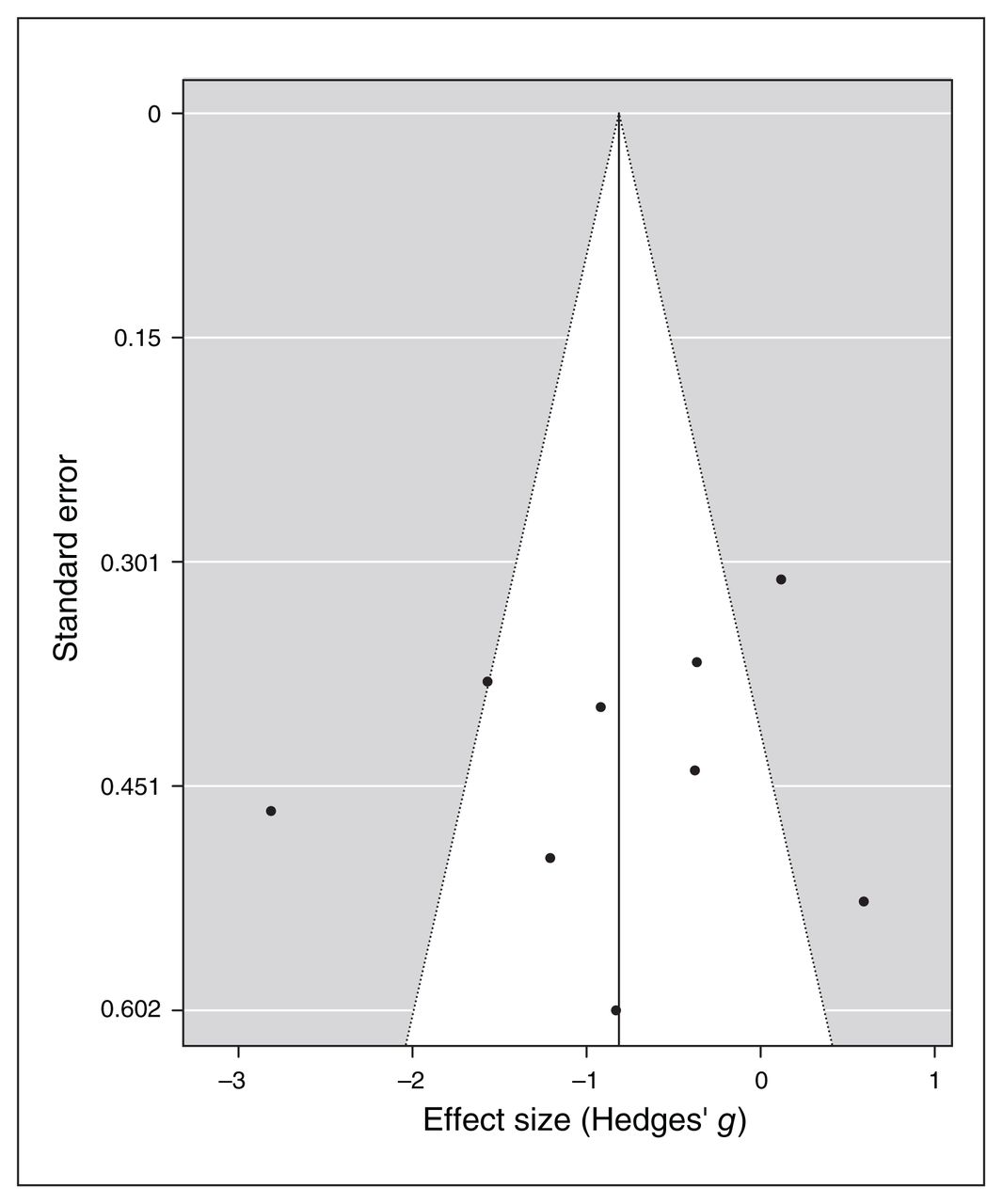
- Figure 8
Publication bias assessed by funnel plot for continuous general anxiety questionnaire scores.
- Figure 9
Forest plot of the effect size of noninvasive brain stimulation on continuous depression questionnaire scores. CI = confidence interval.
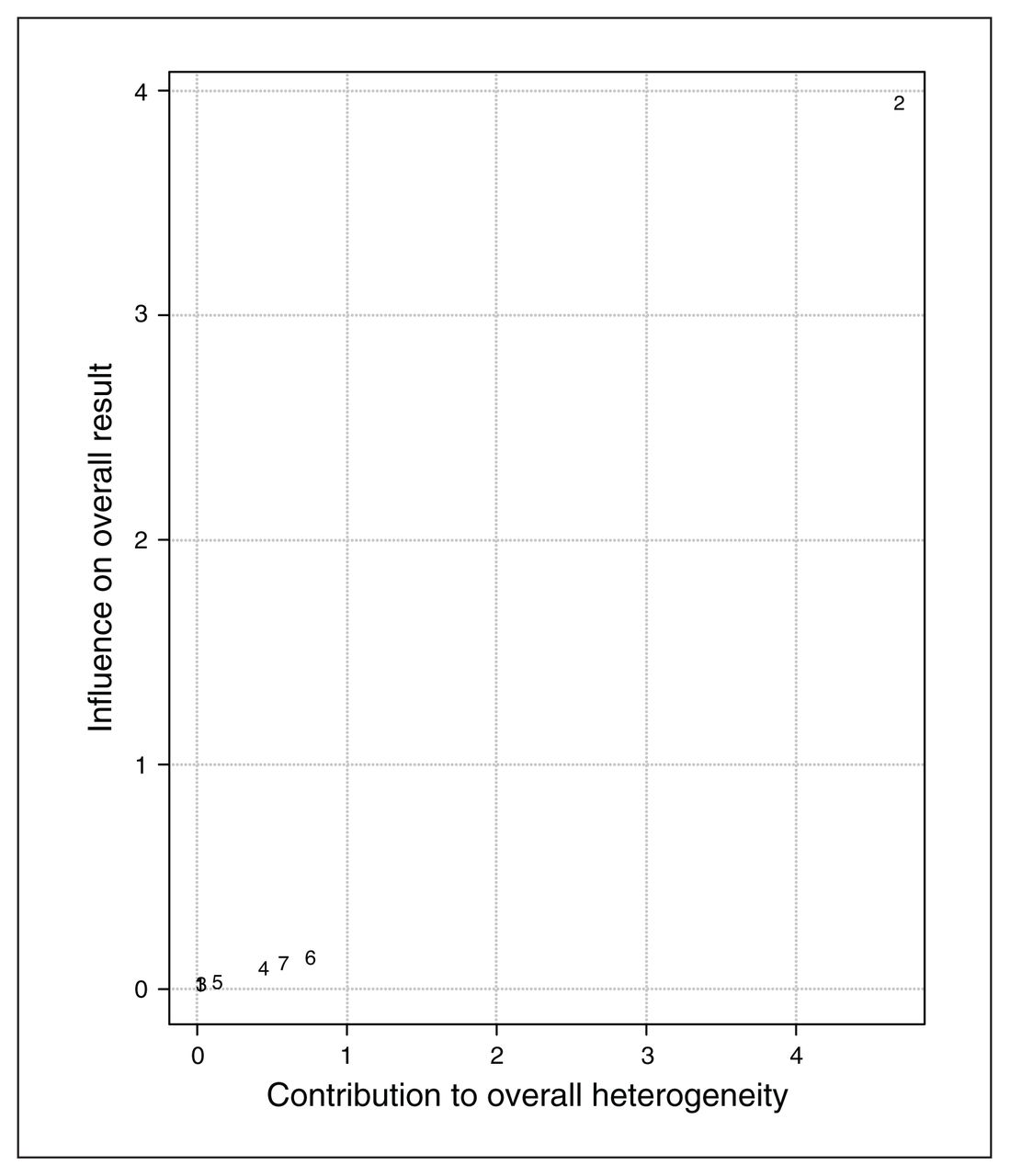
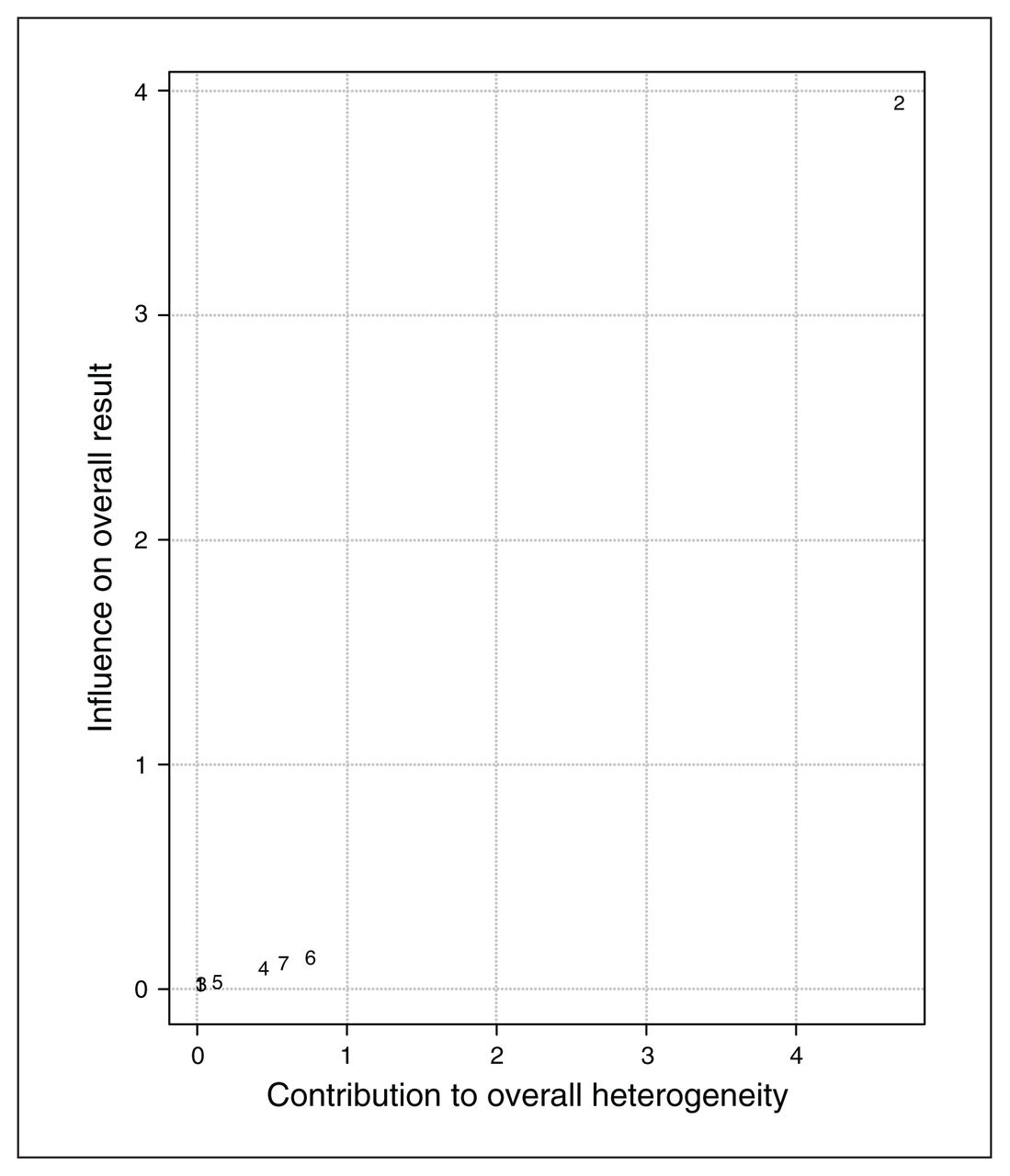
- Figure 10
Baujat plot of study distribution in terms of heterogeneity for continuous depression questionnaire scores. On visual inspection, study 2 (87) seemed to contribute most to the statistical heterogeneity of the included studies.
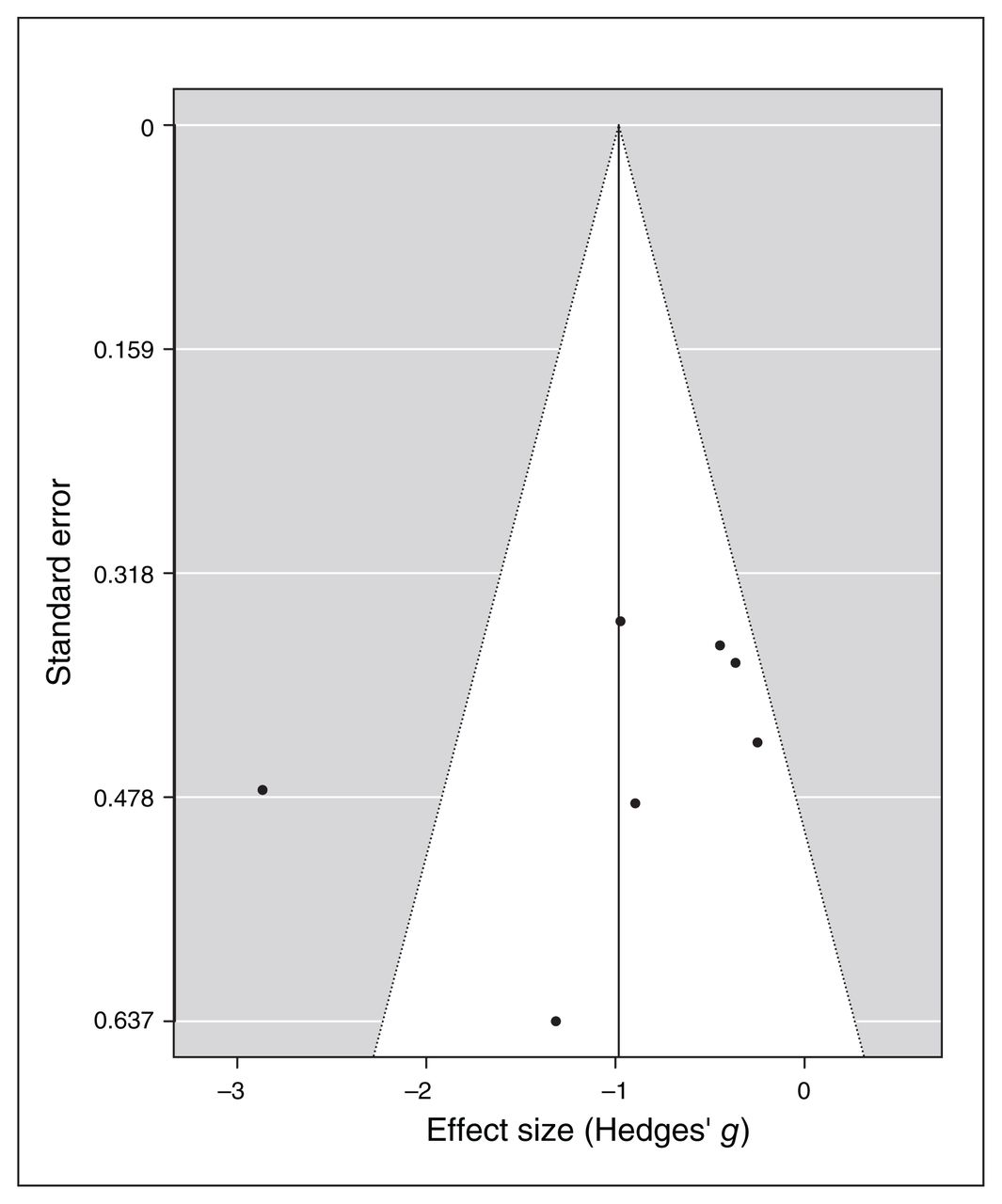
- Figure 11
Publication bias assessed by funnel plot for continuous depression questionnaire scores.






Tables
Sample Outcome measures NIBS Control Study Type No. patients Type No. patients No. sessions Target region Protocol type Blinding Specific anxiety General anxiety Depression De Lima et al. (86) (2019) tDCS 15 Sham 15 5 Left dlPFC Excitatory Double-blind Lipp HAM-A BDI Deppermann et al. (115) (2014) iTBS 20 Sham 21 15 Left dlPFC Excitatory Double-blind PAS HAM-A NR Diefenbach et al. (116) (2016) rTMS 9 Sham 10 10 Right dlPFC Inhibitory Double-blind PSWQ HAM-A HAM-D Dilkov et al. (87) (2017) rTMS 15 Sham 22 25 Right dlPFC Excitatory Double-blind NR HAM-A HAM-D Herrmann et al. (117) (2017) rTMS 20 Sham 19 2 vmPFC Excitatory Double-blind AQ anxiety NR NR Huang et al. (118) (2018) rTMS 18 Sham 18 10 Right PPC Inhibitory Double-blind PSQI HAM-A HAM-D Mantovani et al. (119) (2013) rTMS 11 Sham 10 20 Right dlPFC Inhibitory Double-blind PDSS HAM-A HAM-D Movahed et al. (120) (2018) tDCS 6 Sham 6 10 Right dlPFC Inhibitory Single-blind PSWQ HAM-A HAM-D Nasiri et al. (121) (2020) tDCS 13 UP 15 10 Right dlPFC Inhibitory Double-blind GAD-Q-IV BAI BDI Notzon et al. (88) (2015) iTBS 20 Sham 20 1 Left dlPFC Excitatory Single-blind SPQ NR NR Prasko et al. (122) (2007) rTMS 7 Sham 8 10 Right dlPFC Inhibitory Double-blind PDSS HAM-A NR AQ anxiety = Acrophobia Questionnaire anxiety subscale; BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; dlPFC = left dorsolateral prefrontal cortex; GAD-Q-IV = Generalized Anxiety Disorder Questionnaire-IV; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; iTBS = intermittent theta burst stimulation; Lipp = Lipp Inventory of Stress Symptoms for Adults; NIBS = noninvasive brain stimulation; NR = not reported; PAS = Panic and Agoraphobia Scale; PDSS = Panic Disorder Severity Scale; PPC = posterior parietal cortex; PSQI = Pittsburgh Sleep Quality Index; PSWQ = Penn State Worry Questionnaire; rTMS = repetitive transcranial magnetic stimulation; SPQ = Spider Phobia Questionnaire; tDCS = transcranial direct current stimulation; UP = unified protocol; vmPFC = ventromedial prefrontal cortex.
Cochrane Items Selection bias Performance bias Detection bias Attrition bias Reporting bias Study Random sequence generation Allocation concealment Blinding of participants and personnel Blinding of outcome assessment Incomplete outcome data Selective reporting Other No. of high, %* De Lima et al. (86) (2019) Low Low Low Low Low Low Low 0 Deppermann et al. (115) (2014) High Low Low Low Unsure Low Low 14.29 Diefenbach et al. (116) (2016) High Low Low Low Low Low Low 14.29 Dilkov et al. (87) (2017) Low Low Low Low High Low Low 14.29 Herrmann et al. (117) (2017) High Low Low Low Low Low Low 14.29 Huang et al. (118) (2018) High Low Low Low Low Low Low 14.29 Mantovani et al. (119) (2013) High Low Low Low Low Low Low 14.29 Movahed et al. (120) (2018) High Low High High Low Low Low 42.86 Nasiri et al. (121) (2020) High High Low Low Low High Low 42.86 Notzon et al. (88) (2015) High Low High High Unsure Low Low 42.86 Prasko et al. (122) (2007) High Low Low Low Low Low Low 14.29 ↵* We calculated a percentage for each study, as the quotient of the number of “High” ratings and the total number of relevant items. The lower the percentage, the lower the overall risk of bias.
Stimulation Control Author Age, yr M/F Education Age, yr M/F Education Diagnosis Recruitment De Lima et al. (86) (2019) 32.07 ± 6.5 5/10 2 elementary, 9 secondary, 4 university 29 ± 5.05 6/9 2 elementary, 7 secondary, 6 university GAD Two outpatient clinics Deppermann et al. (115) (2014) 37.6 (range 19–63) 9/13* 12.1 ± 1.7 yr 36.3 (range 22–56) 8/14* 12.4 ± 2.0 yr PD ± agoraphobia Outpatient clinics, advertisements, internet, information sent to local physicians Diefenbach et al. (116) (2016) 44.00 ± 11.95 1/8 12 yr (high school diploma) 44.58 ± 14.75 3/7 12 yr (high school diploma) GAD Outpatient clinic, advertisements, internet, community flyers, physician referral, media coverage Dilkov et al. (87) (2017) 34 ± 7 9/6 NR 38 ± 10 11/11 NR GAD 2 mood disorder centres: Canada and Bulgaria Herrmann et al. (117) (2017) 43.2 ± 12.6 7/13 NR 46.6 ± 13.7 6/13 NR SP Advertisements in local newspapers Huang et al. (118) (2018) 44.94 ± 11.64 9/9 NR 45.22 ± 10.85 9/9 NR GAD + insomnia Neurology outpatient clinic Mantovani et al. (119) (2013) 40.2 ± 10 4/8† NR 39.87 ± 13.3 8/5† NR PD + MDD NR Movahed et al. (120) (2018) NR NR NR NR NR NR GAD NR Nasiri et al. (121) (2020) 20.23 ± 2.89 3/10 NR 21.53 ± 3.56 4/11 NR GAD + MDD University announcements Notzon et al. (88) (2015) 25.85 ± 7.65 20‡ 11.30 ± 3.91 yr 27.02 ± 9.23 20‡ 11.34 ± 3.51 yr SP Local advertisements Prasko et al. (122) (2007) 33.7 ± 9.2 1/6 5 elementary, 1 secondary, 1 university 33.8 ± 12.2 3/5 1 elementary, 6 secondary, 1 university PD NR F = female; GAD = generalized anxiety disorder; M = male; MDD = major depressive disorder; NR = not reported; PD = panic disorder; SP = specific phobia. Values are mean ± standard deviation or n, unless otherwise specified.
↵* The number of males and females was based on the original number of participants included in the study reported in Deppermann et al. (110) (2017). Three participants did not complete the study (2 from the stimulation group and 1 from the sham group), but their sex was not reported by the authors.
↵† The number of males and females was based on the original number of participants included in the study. Four participants did not complete the study (1 from the stimulation group and 3 from the sham group).
↵‡ Participant sex in the stimulation and sham groups were not specified; we have reported the total number of patients from the authors’ data set.
Study Inclusion criteria Exclusion criteria De Lima et al. (86) (2019) GAD diagnosis (DSM-5)
Age 20–30 yrPsychotherapy or hospitalization indication from the psychiatrist at the beginning of the study Deppermann et al. (115) (2014) Age 18–65 yr
PD with or without agoraphobia (DSM-IV-TR)Severe somatic disorders Diefenbach et al. (116) (2016) Age > 18 yr
GAD as principal or coprincipal disorder
HAM-A and HAM-D cut-offUnstable medical/psychiatric condition (e.g., thyroid disease, suicidality)
Current PTSD
Substance use disorder
Lifetime bipolar, psychotic, developmental or obsessive–compulsive disorder
Concurrent psychotherapyDilkov et al. (87) (2017) Age 18–65 yr
GAD primary diagnosis (DSM-IV)Diagnosis of psychotic disorder, bipolar disorder I, MDD or substance/alcohol dependence in the 6 months before the study
Severe axis II disorder
Suicidal
Severe or unstable medical conditions
ECT treatment in the previous 3 mo
TMS treatment in the previous 6 moHerrmann et al. (117) (2017) Specific phobia (acrophobia) diagnosis (DSM-IV)
Subjective motivation to do something about their fear (at least 3 on a scale of 0–10; extreme motivation)
Motion sickness with 3D movies < 4 (scale of 0–10)Heights treatment in the previous 6 mo
Concurrent involvement in psycho-or pharmacotherapyHuang et al. (118) (2018) Age 18–65 yr
GAD primary diagnosis (DSM-IV)
Insomnia for at least 3 monthsHistory of psychiatric diseases except GAD
Concurrent psychotherapy or counsellingMantovani et al. (119) (2013) Age 18–65 yr
PD and MDD primary diagnosis (DSM-IV-TR)
Current episode duration of at least a month
Residual panic attack and MDD symptoms despite medication
Stable medication for 4 wk
Stable psychotherapy for 3 moSuicide risk
History of bipolar disorder, psychotic disorder or substance dependance/abuse in the previous yearMovahed et al. (120) (2018) Age 18–55 yr
GAD diagnosis (DSM-5)
5 points or higher on the 7-item GAD scalePrevious mental illness
Current physical illness
Current psychological or pharmacological medicationNasiri et al. (121) (2020) Age 18–40 yr
GAD primary diagnosis (DSM-5)
Comorbid MDD diagnosis (DSM-5)
No medication use
Speaks Persian fluently
Ability to participate in all assessment and treatment sessionsNeed for immediate medical/therapeutic intervention
Received no more than 8 sessions of CBT-based intervention within the last 5 yr
Psychiatric disorder/substance abuse
Current diagnosis of mental disorders
Opposition to collaboration at any point in research
Suicidality
History of other psychological treatmentNotzon et al. (88) (2015) Age 18–65 yr
Spider phobia (DSM-IV-TR)
At least 16 on the SPQSevere somatic disorder
History of psychiatric disorders except for specific phobia
Psychiatric or psychotropic medicationPrasko et al. (122) (2007) ICD-10 PD with or without agoraphobia
Nonresponders to SRIs (at least 6 wk)
Age 18–45 yrMDD
Suicidality
HAM-D score > 16
Organic psychiatric disorder
History of psychotic disorder in history
Abuse of alcohol or other drugs
Serious somatic disease
Using nonprescribed medicationCBT = cognitive behavioural therapy; DSM = Diagnostic and Statistical Manual of Mental Disorders; ECT = electroconvulsive therapy; GAD = generalized anxiety disorder; HAM-A = Hamilton Anxiety Rating Scale; HAM-D = Hamilton Depression Rating Scale; MDD = major depressive disorder; NR = not reported; PD = panic disorder; PTSD = posttraumatic stress disorder; SP = specific phobia; SPQ = Spider Phobia Questionnaire; SRI = serotonin reuptake inhibitor; TMS = transcranial magnetic stimulation; TR = text revision.
- Table 5
Summary of stimulation protocols details, treatment strategies and associated therapies
Study Intensity Duration Coil/electrode position tDCS reference Sham procedure Psychological intervention Treatment strategy Medication De Lima et al. (86) (2019) 2 mA
Electrode size 5 × 720 min F3 FP2 30 s Not allowed Monotherapy Stable doses Deppermann et al. (115) (2014) 15 Hz
80% rMT3 min; 18 trains of 2 s F3 – 90° from skull Psychoeducation, 3 group sessions Monotherapy Stable doses for 3 wk Diefenbach et al. (116) (2016) 1 Hz
90% rMT15 min; 900 pulses per session Individual structural MRI: x, y, z = 42, 36, 32 (MNI) – Sham coil Not allowed Monotherapy Stable doses for 3 mo or stable benzodiazepines for 2 wk Dilkov et al. (87) (2017) 20 Hz
110% rMT20 trains, 9 s per train; 51 s intertrain interval 5 cm rostral to motor cortex – 90° from skull, same intensity Allowed Monotherapy Stable doses for 6 mo or no medications for at least 2 wk Herrmann et al. (117) (2017) 10 Hz
100% rMT40 trains of 4 s (1560 pulses; intertrain interval 26 s FPZ – Sham coil Virtual reality exposure Augmentation Not allowed Huang et al. (118) (2018) 1 Hz
90% rMT3 trains of 500 pulses; intertrial interval 10 min P4 – Sham coil Not allowed Monotherapy Stable doses for 3 mo Mantovani et al. (119) (2013) 1 Hz
110% rMT30 min 5 cm anterior to motor cortex – Sham coil Allowed Monotherapy Stable doses for 4 wk or no medication for 6–8 wk before Movahed et al. (120) (2018) 2 mA
Electrode size NR20 min F4 Left deltoid NR Not allowed Monotherapy Not allowed Nasiri et al. (121) (2020) 2 mA
Electrode size 5 × 530 min F4 Left deltoid F3 UP 12 sessions Monotherapy Not allowed Notzon et al. (88) (2015) 15 Hz
80% rMT3 min; 18 trains of 2 s F3 – 90° from skull Virtual reality exposure Augmentation Not allowed Prasko et al. (122) (2007) 1 Hz
110% rMT30 min 5 cm rostral to motor cortex – 90° from skull, same intensity NR Monotherapy Stable doses EEG = electroencephalogram; F3 = 10–20 EEG position corresponding to the left dorsolateral prefrontal cortex; F4 = 10–20 EEG position corresponding to the right dorsolateral prefrontal cortex; FP2 = 10–20 EEG position corresponding to the supraorbital region; FPZ = 10–20 EEG position corresponding to the ventromedial prefrontal cortex; MNI = Montreal Neurological Institute; NR = not reported; P4 = 10–20 EEG position corresponding to the right posterior parietal cortex; rMT = resting motor threshold; UP = unified protocol.
- Table 6
Summary of stimulation protocol, statistical analyses, main results and additional groups and measures (part 1 of 2)
Study Protocol Follow-up Statistical analysis Reported results Additional groups Additional pre/post measures De Lima et al. (86) (2019) 5 consecutive days 1 wk ANOVA repeated-measures Anxiety and depression symptoms did not differ between real and sham tDCS. Physical symptoms of stress were reduced at the end of treatment and at follow-up in the tDCS group v. the sham group None Anxiety: BAI Global evaluation: PANAS Deppermann et al. (115) (2014) 5 daily sessions; 3 wk NR ANOVA repeated-measures No differences in real v. sham rTMS. Both groups showed improvement in anxiety symptoms post-iTBS v. baseline Healthy controls; only for fNIRS Physiological: CAQ Brain activation: fNIRS Cognitive: verbal fluency Diefenbach et al. (116) (2016) 5 daily sessions; 6 wk 3 mo, 6 mo (only a subset not included in statistical analysis) ANOVA repeated- measures; planned contrasts Anxiety symptoms improved in post- v. pre- measurements in rTMS and sham groups that persisted at 3 mo follow-up only in the rTMS group. Worry and depressive symptoms improved only in the rTMS group at the end of treatment and at 3 mo follow-up. Brain activation increased after rTMS and tended to decrease after sham None Anxiety/mood: DASS-DEP Brain activation: fMRI during gambling task Dilkov et al. (87) (2017) 6 wk; 5 sessions/wk for the first 4 wk; during the wk 5, sessions reduced to 3 times/wk; during wk 6, sessions reduced to 2 times/wk 2 wk and 6 wk after the end of treatment ANOVA repeated-measures Anxiety and depressive symptoms improved in the stimulation v. sham condition at the end of treatment and the 2 follow-ups None Global evaluation: CGI Herrmann et al. (117) (2017) 2 sessions 3 mo ANOVA repeated-measures; t test 2 sessions of rTMS reduced anxiety and avoidance ratings compared to the sham group None Anxiety: AQ-avoidance subscale; BAT Huang et al. (118) (2018) 10 consecutive days 2 wk, 1 mo ANOVA repeated- measures Anxiety, insomnia and depressive symptoms improved in the rTMS group v. the sham group at the end of treatment and the 2 follow-ups None NR Mantovani et al. (119) (2013) 5 d/wk; 4 wk double- blind + 4 weeks real* 1, 3 and 6 mo ANOVA repeated- measures; t test 4 weeks rTMS v. sham: improvement in panic symptoms but not depression. 8 weeks of rTMS v. pre- treatment: improvement in panic and depressive symptoms, global assessment, and social adjustment None Anxiety: PDSS, PDSS-SR Mood: BDI; ZUNG-SAS Global evaluation: CGI; PGI; SASS Movahed et al. (120) (2018) 4 wk 2 mo ANOVA repeated- measures Worry, anxiety and depression scores were reduced after cathodal tDCS and pharmacotherapy v. sham tDCS. Pharmacotherapy was stronger than tDCS in reducing worry; tDCS was stronger in reducing depression. Anxiety symptoms did not differ after cathodal tDCS compared to pharmacotherapy Pharmacotherapy NR Nasiri et al. (121) (2020) 10 daily sessions; 2 wk 3 mo MANCOVA Worry, anxiety and anxiety sensitivity improved after UP + tDCS v. UP alone at the end of treatment and at follow-up Waiting list Anxiety: ASI; IUS; PSWQ Notzon et al. (88) (2015) Single session NR ANOVA repeated- measures iTBS increased sympathetic activity during the spider scene in both phobic and healthy participants Healthy controls (real and sham) Anxiety: FSQ; ASI Global evaluation: IPQ; SUDS; DS Physiological: HR; SCL Brain activation: fNIRS Prasko et al. (122) (2007) 5 daily sessions; 2 wk 2 wk Nonparametric repeated- measures ANOVA Anxiety symptoms and psychopathology global scores improved after both real and sham rTMS None Anxiety: BAI Global evaluation: CGI ANOVA = analysis of variance; AQ = Acrophobia Questionnaire; ASI = Anxiety Sensitivity Index; BAI = Beck Anxiety Inventory; BAT = Behavioral Avoidance Test; BDI = Beck Depression Inventory; CAQ = Cardiac Anxiety Questionnaire; CGI = Clinical Global Impression Scale; DASS-DEP = Depression-Anxiety Scales Depression Subscale; DS = Disgust Scale; fMRI = functional magnetic resonance imaging; fNIRS = functional near-infrared spectroscopy; FSQ = Fear of Spiders Questionnaire; HR = heart rate; IPQ = Igroup Presence Questionnaire; iTBS = intermittent theta burst stimulation; IUS = Intolerance of Uncertainty Scale; MANCOVA = multivariate analysis of covariance; NR = not reported; PANAS = Positive and Negative Affect Schedule; PDSS(−SR) = Panic Disorder Severity Scale (self-report); PGI = Patient Global Impression; PSWQ = Penn State Worry Questionnaire; rTMS = repetitive transcranial magnetic stimulation; SASS = Self-reported Social Adaptation Scale; SCL = skin conductance level; SUDS = Subjective Units of Discomfort Scale; tDCS = transcranial direct current stimulation; UP = unified protocol; ZUNG-SAS= Zung-Self Administered Scale.
↵* In our analysis, we included data for the baseline and the first 4 weeks of rTMS treatment.
Comparison No. of studies Effect size summary (95% confidence interval) Z Q test I2 (%) Influence test Egger’s test Kendall’s rank test Specific anxiety 9 −0.4858 (−0.8319 to −0.1398) −2.7517
p = 0.00617.6384
p = 0.04048.98 None −1.2078
p = 0.23−0.2889
p = 0.29General anxiety 9 0.8139 (−1.4484 to −0.1794) −2.5142
p = 0.01241.0326
p < 0.00180.50 Dilkov et al. (87) (2017) −0.3108
p = 0.76−0.1667
p = 0.61General anxiety* 8 −0.5684 (−1.0626 to −0.0742) −2.2541
p = 0.02419.5887
p = 0.00764.27 None −0.1009
p = 0.92−0.1429
p = 0.72Depression 7 −0.9822 (−1.6177 to −0.3468) −3.0297
p = 0.00223.4602
p < 0.00174.42 Dilkov et al. (87) (2017) −0.9869
p = 0.32−0.1429
p = 0.77Depression* 6 −0.6433 (−0.9786 to −0.3081) −3.7616
p < 0.0013.8846
p = 0.57– None −0.7960
p = 0.43−0.0667
p > 0.99↵* Indicates results after outlier removal.
- Table 8:
Results of the moderation analysis for specific and general anxiety scores and depression scores
Moderator SMD (95% CI) z p Q1 Specific anxiety measure Session number −0.0414 (−0.1038 to 0.0209) −1.3019 0.19 1.6950 Technique −0.2827 (−0.7443 to 0.1788) −1.2006 0.23 1.4415 Target region −0.4963 (−1.2778 to 0.2852) −1.2447 0.21 1.5493 Protocol type −0.4965 (−1.1366 to 0.1435) −1.5205 0.13 2.3118 General anxiety measure Session number −0.0723 (−0.1811 to 0.0364) −1.3039 0.19 1.7001 Technique −0.1830 (−1.2449 to 0.8790) −0.3377 0.74 0.1140 Target region −0.8212 (−2.2992 to 0.6568) −1.0890 0.28 1.1858 Protocol type 0.2243 (−1.2106 to 1.6592) 0.3064 0.76 0.0939 Depression measure Session number −0.0777 (−0.1634 to 0.0080) −1.7760 0.076* 3.1542 Technique 0.5794 (−0.7260 to 1.8847) 0.8699 0.38 0.7567 Target region −0.6709 (−2.9417 to 1.5998) −0.5791 0.56 0.3354 Protocol type 0.8540 (−0.5639 to 2.2718) 1.1805 0.24 1.3935 Comorbidity 0.9563 (−0.3677 to 2.2803) 1.4157 0.16 2.0042 CI = confidence interval; dlPFC = dorsolateral prefrontal cortex; iTBS = intermittent theta burst stimulation; rTMS = repetitive transcranial magnetic stimulation; SMD = standardized mean difference (effect size); tDCS = transcranial direct current stimulation. The applied technique (iTBS, rTMS, tDCS), target region (left vs. right dlPFC) and protocol type (excitatory v. inhibitory) moderators were categorical variables; session number was a numerical variable. For the depression outcome measure only, we computed whether the presence of comorbid depression influenced the outcome of the scores. z = z score associated with the SMD value; p = p value associated with the z score in the same row.
↵* p < 0.10.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





