

Abstract
Background Subcortical volumetric abnormalities in schizophrenia, bipolar disorder and major depressive disorder (MDD) have been consistently found on a single-diagnosis basis in previous studies. However, whether such volumetric abnormalities are specific to a particular disorder or shared by other disorders remains unclear.
Methods We analyzed the structural MRIs of 160 patients with schizophrenia, 160 patients with bipolar disorder, 160 patients with MDD and 160 healthy controls. We calculated the volumes of the thalamus, hippocampus, amygdala, accumbens, putamen, caudate, pallidum and lateral ventricles using FreeSurfer 7.0 and compared them among the groups using general linear models.
Results We found a significant group effect on the volumes of the thalamus, hippocampus, accumbens and pallidum. Further post hoc analysis revealed that thalamic volumes in patients with schizophrenia, bipolar disorder and MDD were significantly reduced compared to those in healthy controls, but did not differ from one another. Patients with schizophrenia and bipolar disorder also shared a significant reduction in hippocampal volumes. Among the 3 clinical groups, patients with schizophrenia showed significantly lower hippocampal volumes and higher pallidal volumes than patients with bipolar disorder and MDD.
Limitations Differences in psychotropic use and duration of illness among the patient groups may limit the interpretation of our findings.
Conclusion Our findings indicate that decreased thalamic volume is a common feature of schizophrenia, bipolar disorder and MDD. Smaller hippocampal and larger pallidal volumes differentiate schizophrenia from bipolar disorder and MDD and may provide clues to the biological basis for the Kraepelinian distinction between these illnesses.
Introduction
Schizophrenia, bipolar disorder and major depressive disorder (MDD) are severe mental illnesses that have a considerable negative effect on sensory or affective processing, cognitive function and social function. Diagnosis of these disorders originates from the classical Kraepelinian division of dementia precox (schizophrenia) and manic–depressive illness (bipolar disorder).1 In modern psychiatry, categorical diagnosis is made based on symptoms and clinical features listed in the most recent version of the Diagnostic and Statistical Manual of Mental Disorders.2 However, recent meta-analyses and cross-disorder imaging studies have provided evidence that these psychiatric disorders may share common brain abnormalities. A meta-analysis of 193 voxel-based morphometry (VBM) studies comparing 15 892 individuals across 6 diverse diagnostic groups (schizophrenia, bipolar disorder, MDD, substance addiction, obsessive–compulsive disorder and anxiety disorder) with matched controls revealed that grey matter loss converged across diagnoses in 3 regions: the dorsal anterior cingulate cortex and the bilateral insula.3 Another meta-analysis of VBM studies revealed that bipolar disorder and MDD share common grey matter deficits in the dorsomedial and ventromedial prefrontal cortex, including the anterior cingulate cortex and bilateral insula.4
As well, increasing numbers of studies have adopted a transdiagnostic approach, recruiting patients with various psychiatric disorders to the same study, and have indicated the potential to directly identify common neural substrates across disorders. One study demonstrated that both bipolar disorder and schizophrenia presented with substantial volume reductions in the thalamus, hippocampus and nucleus accumbens,5 and suggested a common underlying subcortical pathophysiology. A VBM study that included patients with first-episode psychosis, MDD, posttraumatic stress disorder and obsessive–compulsive disorder found that enlargement of the putamen was common to these 4 groups of patients.6 A cross-disorder study that included different psychiatric disorders could help delineate common and distinct neural abnormalities in these disorders.
Subcortical structures may play a vital role in the pathogenesis of psychiatric disorders because of their extensive cortico-subcortical circuits. These circuits have abundant neurons that produce major neural modulators, such as dopamine, serotonin and norepinephrine, which are the targets of various psychotropic medications. Subcortical volumetric abnormalities have been well studied on a single-diagnosis basis and have been demonstrated in a range of psychiatric disorders.
In a large meta-analysis,7 schizophrenia was associated with reduced volumes in the thalamus, hippocampus and amygdala, and with enlarged structures in the pallidum and putamen. A stronger leftward asymmetry of the volume of the pallidum in schizophrenia has also been reported.8 Bipolar disorder has been associated with reduced volumes in the thalamus and hippocampus.9 MDD has been associated with reduced volumes in the hippocampus,10 thalamus11 and putamen.11 A large meta-analysis using shape analysis also demonstrated that patients with adolescent-onset MDD had lower thickness and surface area in hippocampal subfields and the basolateral amygdala.12 Notably, a recent study involving people with an at-risk mental state revealed volume expansion in the caudate and globus pallidus, suggesting that subcortical volumetric abnormalities cannot be explained by medication effects only and might be related to a general vulnerability to psychopathology.13 Together, these findings confirm the vital role of subcortical structures in major psychiatric disorders. However, a limitation of these studies is that they focused on only a single disorder, making it less clear if such volumetric abnormalities are specific to a particular disorder or shared by several.
In the present study, we used a single-site data set to evaluate subcortical volumes in patients with 3 major psychiatric disorders (schizophrenia, bipolar disorder and MDD) and to test the hypothesis that common subcortical volumetric abnormalities exist and extend across diagnoses. We focused on 7 structures: the thalamus, hippocampus, amygdala, putamen, caudate, accumbens and pallidum. We collected data using the same MRI machine and acquisition parameters between 2010 and 2019, minimizing the potential confounding effects of medical centre, MRI machine and acquisition parameters compared to previous large-scale meta-analysis studies. In addition to identifying common deficits, we also aimed to identify volumetric differences among these 3 major psychiatric disorders and understand possible biological substrates for diagnostic classification.
Methods
Participants
In the present study, we included 160 patients with schizophrenia, 160 patients with bipolar disorder (145 patients with bipolar I and 15 patients with bipolar II), 160 patients with MDD and 160 healthy controls. Participant ages ranged from 18 to 64 years. We selected participants from a single-site MRI data set to match the age and sex of the 4 groups as much as possible; however, we could not match the MDD sample to the other groups by sex because of the high number of women in the data set. The MDD group also had a shorter duration of illness than the schizophrenia and bipolar disorder groups because we matched participants by age; we could not match duration of illness at the same time because MDD had a later onset.
Participants with schizophrenia, bipolar disorder and MDD were recruited from outpatient and inpatient units of the Taipei Veterans General Hospital in Taiwan, and diagnoses were based on the DSM-IV.14 Participants were screened to exclude those with the following conditions: substance abuse or dependence issues over the preceding 6 months; a history of head injuries that resulted in sustained loss of consciousness, cognitive sequelae or both; and neurologic illness or any other disorder that affects cerebral metabolism. We characterized the clinical status of patients with schizophrenia using the Positive and Negative Syndrome Scale.15 We conducted clinical assessments of patients with bipolar disorder and MDD using the Young Mania Rating Scale and the Montgomery–Åsberg Depression Rating Scale, but not all patients received complete ratings. Before they participated in the experiment, patients were receiving treatment with various medications, including atypical antipsychotics, antidepressants, antiepileptics and lithium.
Healthy controls were recruited via advertisements. An experienced psychiatrist used the Mini International Neuropsychiatric Inventory Plus16 to screen and exclude candidates with major psychiatric illnesses. Candidates with first-degree relatives who had Axis I disorders, including schizophrenia, bipolar disorder and MDD, were also excluded.
All procedures were approved by the Institutional Review Board of Taipei Veterans General Hospital, and all participants provided written informed consent.
MRI acquisition
We acquired all participants’ structural images using the same MRI machines with the same acquisition parameters. We acquired MRI images using a 3.0 T GE Discovery 750 whole-body high-speed imaging device with an 8-channel brain coil (repetition time 2530 ms, echo spacing 7.25 ms, echo time 3 ms, flip angle 7°, isotropic 1 mm voxel, field of view 256 × 256). The total acquisition time was 5 minutes and 59 seconds. We used cushioning for head stabilization, and all participants wore earplugs (29 dB rating) for noise attenuation.
Image processing and subcortical volumetry
We analyzed all structural T1 images using FreeSurfer version 7.0 (www.nmr.mgh.harvard.edu/martinos).17 Images were preprocessed using a standard automatic reconstruction algorithm, and we calculated the volumes of the thalamus, caudate, putamen, pallidum, accumbens, hippocampus and amygdala for statistical analysis. We also evaluated the lateral ventricles and intracranial volume (ICV) because they have been frequently reported in previous studies, and ICV is an essential covariate in between-group comparisons of subcortical volume.
We initially collected and evaluated the MRI images of 927 participants (222 patients with schizophrenia, 263 patients with bipolar disorder, 190 patients with MDD and 252 healthy controls). We visually inspected all images and excluded those of 20 participants because of motion artifacts, susceptibility artifacts or segmentation failure. Then, we selected 160 participants for each group according to their demographic properties.
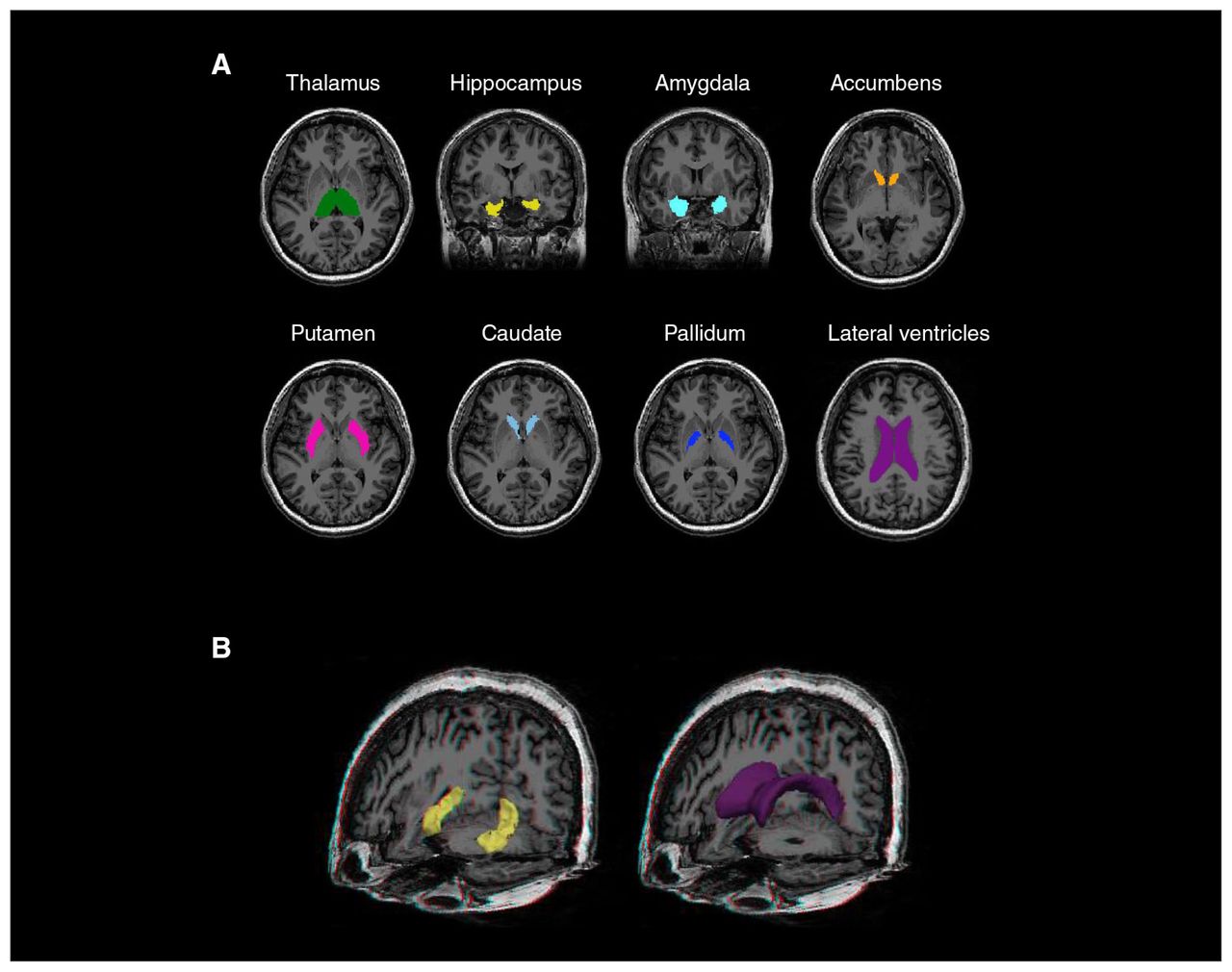
We assessed data quality using the Qoala-T Tool (https://github.com/Qoala-T/Qoala-T),18 which uses a supervised learning model to rate the quality of FreeSurfer-preprocessed scans. The data from all 640 participants had a Qoala-T score of greater than 50% and were included for statistical analysis. Figure 1 presents an example of the 8 subcortical structures segmented using FreeSurfer in a healthy control participant.

Subcortical structures evaluated in this study. (A) An example of the subcortical segmentations examined using FreeSurfer 7.0 in a healthy control participant. (B) The hippocampus and lateral ventricles were delineated in a 3-dimensional view for better visualization of their whole structures.
Statistical analysis
We performed statistical analyses using SPSS version 20 (IBM). We examined differences in demographic characteristics among the 4 groups using the χ2 test for categorical variables and analysis of variance for continuous variables.
We averaged the volumes of the left and right subcortical structures for statistical analysis. For each subcortical structure, we examined group difference in volumes using a univariate general linear model, where volume was the outcome measure, an indicator of diagnosis (1 = MDD, 2 = bipolar disorder, 3 = schizophrenia, 4 = healthy control) was the predictor of interest, and age, sex and ICV were covariates of no interest. If we found a significant effect of diagnosis, we performed post hoc comparisons to understand the volumetric differences among the 4 participant groups. We have reported uncorrected p values with a significance threshold determined by Bonferroni correction (p = 0.05/9 = 0.0056 for the main effect and p = 0.05/6 = 0.0083 for post hoc pair-wise comparisons). We also estimated the effect sizes (Cohen d) of each patient group compared to healthy controls, adjusted for age, sex and ICV, using the t statistic from the independent variable of diagnosis.19
To understand the effects of illness duration and symptom severity on subcortical volumes in the 3 patient groups, we used partial correlations to evaluate the association between these clinical variables and subcortical volumes using Spearman correlation coefficients and age, sex, ICV and psychotropic use (4 dummy variables for antipsychotics, antidepressants, antiepileptics and lithium) as covariates of no interest. We defined symptom severity using the Positive and Negative Syndrome Scale total score in patients with schizophrenia, the Young Mania Rating Scale score in patients with bipolar disorder and the Montgomery–Åsberg Depression Rating Scale score in patients with MDD. We added duration of illness as a covariate in evaluating the correlation between symptom severity and subcortical volumes. In total, we performed 42 comparisons (7 structures × 2 clinical variables × 3 diagnostic groups) and determined the significance threshold by Bonferroni correction (p = 0.05/42 = 0.0012).
Results
Demographic and clinical characteristics
Table 1 lists participant demographic and clinical characteristics. The mean ± standard deviation (SD) ages of participants did not differ by group: schizophrenia 37.0 ± 8.8 years; bipolar disorder 37.8 ± 11.5 years; MDD 36.8 ± 11.9 years; and healthy controls 36.6 ± 8.0 years. As noted above, the MDD group could not be sex-matched to the other groups because it contained a high number of women. Mean illness durations for patients with schizophrenia, bipolar disorder and MDD were 13.2 ± 9.1, 12.6 ± 8.9 and 6.7 ± 6.8 years, respectively.
Participant demographic and clinical characteristics
Group differences in subcortical volumes
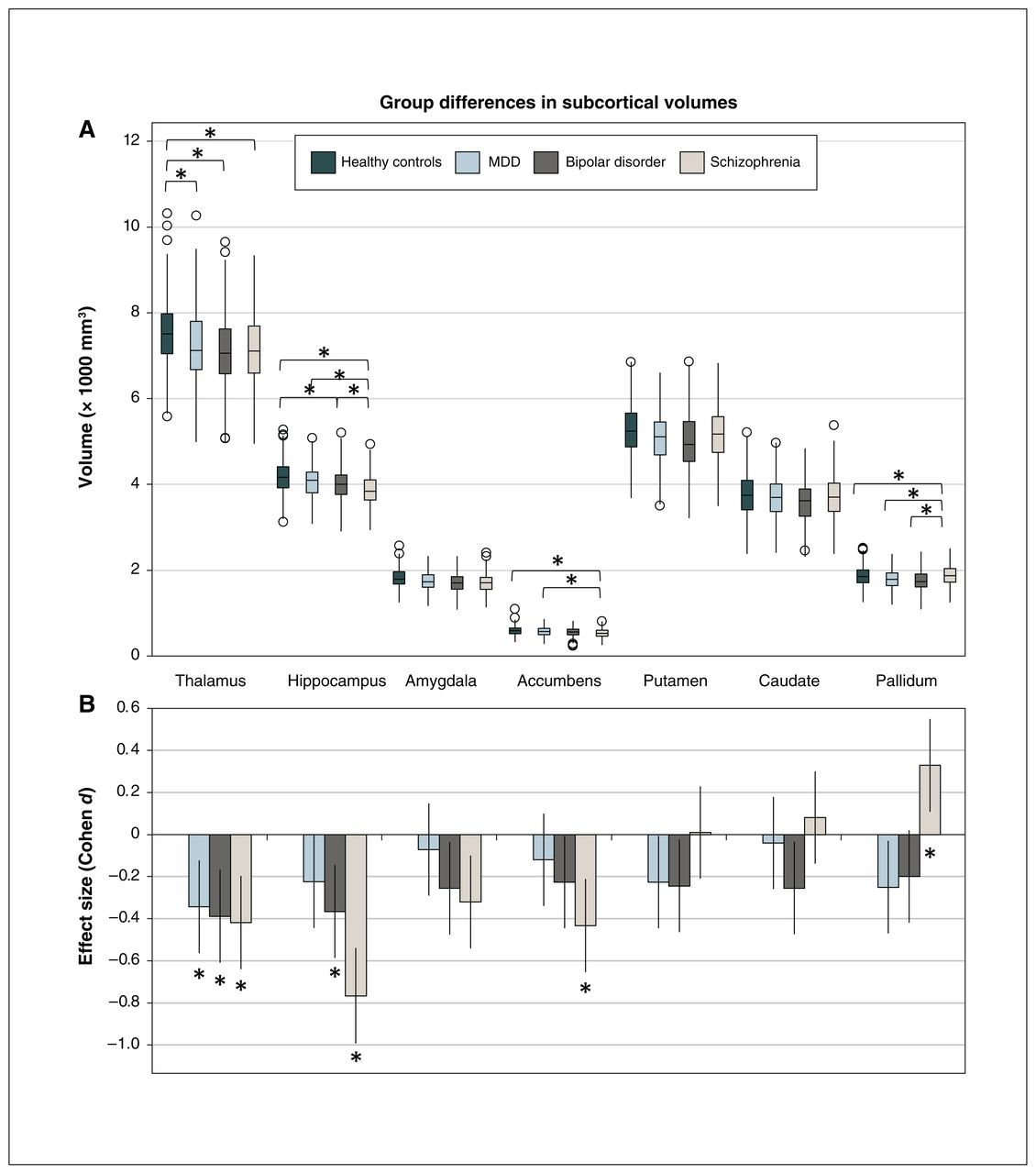
Detailed statistical findings for group differences in subcortical volumes are shown in Table 2 and Figure 2A.
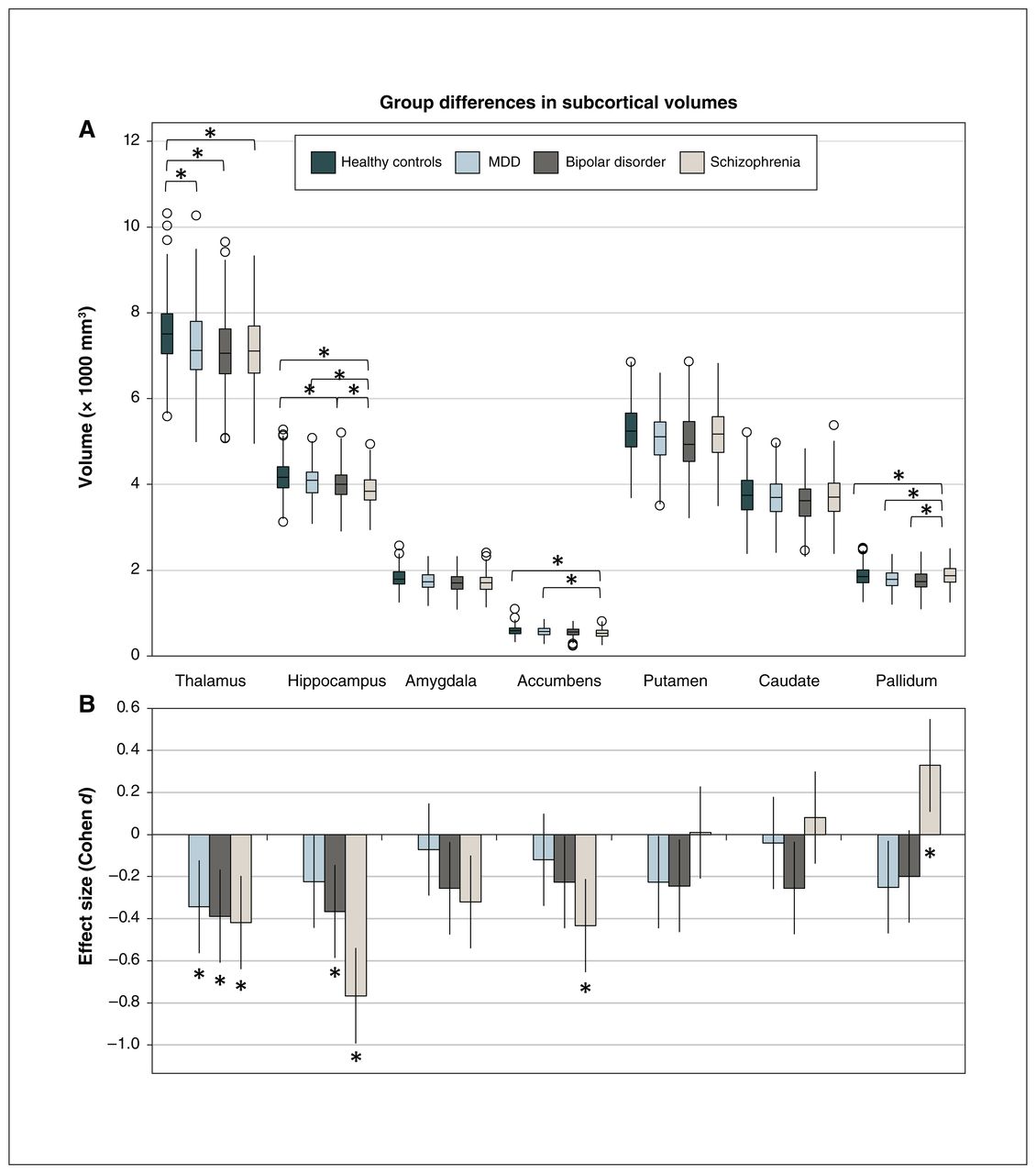
Common and distinct subcortical volumetric abnormalities in patients with schizophrenia, bipolar disorder and MDD. (A) We assessed the model-adjusted volumes of the subcortical structures (mean ± standard deviation) for each diagnostic group and evaluated differences among the 4 diagnostic groups using general linear models; *p < 0.05 (Bonferroni-corrected) in post hoc comparisons. (B) We calculated the effect size (Cohen d) and 95% confidence interval for differences in subcortical volume between each patient group and healthy controls to better visualize common volumetric abnormalities. Decreased thalamic volume was a common feature of the 3 disorders; *p < 0.05 (Bonferroni-corrected) compared to healthy controls. MDD = major depressive disorder.
Subcortical volume and group differences, general linear models
We observed a significant difference across all diagnostic groups in the thalamus (F3,633 = 6.0, p < 0.001), hippocampus (F3,633 = 16.5, p < 0.001), accumbens (F3,633 = 5.3, p = 0.001) and pallidum (F3,633 = 10.9, p < 0.001). Further post hoc comparisons demonstrated that patients with schizophrenia (d = −0.42, p < 0.001), bipolar disorder (d = −0.39, p = 0.001) and MDD (d = −0.35, p = 0.002) had significantly lower thalamic volumes than healthy controls, but the clinical groups did not differ from one another.
Patients with schizophrenia (d = −0.77, p < 0.001) and bipolar disorder (d = −0.37, p = 0.001) exhibited a significant reduction in hippocampal volume compared to healthy controls; the reduction observed in patients with MDD was not significant (d = −0.23, p = 0.046). Patients with schizophrenia also had significantly lower hippocampal volumes than patients with bipolar disorder (d = −0.54, p < 0.001) and MDD (d = −0.41, p < 0.001), suggesting a more severe volumetric deficit in schizophrenia.
Patients with schizophrenia showed significantly lower volumes in the accumbens than healthy controls (d = −0.44, p < 0.001) and patients with MDD (d = −0.31, p = 0.006). Patients with schizophrenia also exhibited significantly higher volumes in the pallidum than healthy controls (d = 0.33, p = 0.003), patients with bipolar disorder (d = 0.53, p < 0.001) and patients with MDD (d = 0.58, p < 0.001).
In summary, the 3 major psychiatric disorders shared a common feature of decreased thalamic volume. Larger pallidal and smaller hippocampal volumes differentiated schizophrenia from bipolar disorder and MDD. For visualization of these common volumetric abnormalities, Cohen d effect sizes and 95% confidence intervals for differences in subcortical volumes between groups are shown in Figure 2B.
To control for the potential effects of psychotropic use and illness duration on our findings, we performed an analysis in which we added these variables as additional covariates (antipsychotics, antidepressants, antiepileptics and lithium as 4 dummy variables). The findings of the control analysis still revealed a significant difference across the 3 clinical groups for the volumes of the hippocampus (F2,469 = 7.17, p = 0.001) and pallidum (F2,469 = 8.01, p < 0.001), but not the accumbens (F2,469 = 1.82, p = 0.16).
To evaluate potential hemispheric differences in subcortical volumetric abnormalities across the 3 clinical groups, we conducted a supplementary analysis that compared left and right subcortical structures separately (detailed results in Appendix 1, Table S1, available at www.jpn.ca/lookup/doi/10.1503/jpn.210154/tab-related-content). Several of our findings related to the pallidum and accumbens were hemisphere-specific. Patients with schizophrenia had significantly higher volumes in the left and right pallidum than patients with bipolar disorder and MDD, but only showed significantly higher volumes in the left pallidum compared to healthy controls. Furthermore, patients with schizophrenia only showed significantly lower volumes in the right accumbens compared to patients with MDD and healthy controls.
Correlation analysis with clinical features
After correcting for multiple comparisons, we found no significant correlation between subcortical volumes and illness duration or symptom severity in the 3 clinical groups. The detailed results of correlation analysis are shown in Appendix 1, Table S2.
Discussion
In the present study, we evaluated the volumes of major subcortical structures in patients with schizophrenia, bipolar disorder and MDD to identify common and distinct abnormalities in these 3 major psychiatric disorders. Thalamic volume was decreased in all 3 patient groups, and we found no significant difference among them, implying a neural deficit that was common to all. This finding was consistent with our hypothesis that common subcortical volumetric abnormalities exist and extend across diagnoses. The schizophrenia, bipolar disorder, and MDD groups exhibited graded reductions in hippocampal volumes, and hippocampal volume was significantly lower in the schizophrenia group than in the bipolar disorder and MDD groups. In contrast, the schizophrenia group had a significantly higher pallidal volume than the bipolar disorder and MDD groups. These differences in hippocampal and pallidal volumes among the 3 patient groups were still significant after controlling for psychotropic use and duration of illness. The correlation between structural volume and symptom severity was more significant in the MDD group; decreased thalamic and accumbens volumes were associated with more severe depression.
The thalamus plays a crucial role in the organization of cortical and subcortical functions through its wide connections with the cortex, limbic system, basal ganglion and cerebellum. Deficits in thalamus function may contribute to sensory, cognitive and affective symptoms in various psychiatric disorders. For example, a follow-up study of patients with 22q11.2 micro deletion syndrome (30%–35% of whom eventually developed schizophrenia) demonstrated that patients with auditory hallucinations had hyperconnectivity between the thalamus and cortical areas devoted to the primary processing of hearing and to the Wernicke area.20
The role of the thalamus in schizophrenia has been studied extensively. For example, a large-scale follow-up study of first-episode schizophrenia revealed that the size of the thalamus was already decreased in patients with first-episode schizophrenia, and that it continued to decrease after illness onset.21 Consistent with our findings, decreased thalamic volume was observed in patients with schizophrenia as well as patients with bipolar disorder in a cross-disorder study,5 and in a meta-analysis of VBM studies.22 As well, a previous meta-analysis23,24 reported lower thalamic volumes in patients with MDD. The present study demonstrated that the decreased thalamic volume we observed in the 3 patient groups (schizophrenia, bipolar disorder and MDD) was the main subcortical abnormality shared by these 3 major disorders.
The hippocampus is a major structure of the limbic system, and hippocampal volume deficits have been implicated in early-onset psychosis,25 schizophrenia,7 bipolar disorder9 and MDD.4,10 In the present study, patients with schizophrenia and bipolar disorder had decreased hippocampal volumes; in patients with MDD, the reduction was not significant. This finding may have been because patients with MDD in the present study had a later illness onset and a shorter duration of illness; a large-scale study indicated that reductions in hippocampal volume were present mainly in recurrent and early-onset (≤ 21 yr) MDD, absent in patients with a first episode and less pronounced in patients with a late onset of illness (> 21 yr).10
Consistent with our findings, several studies have provided evidence of more severe hippocampal deficits in schizophrenia. Rimol and colleagues5 reported a nonsignificant trend of lower hippocampal volumes in schizophrenia compared to bipolar disorder. Furthermore, Meisenzahl and colleagues26 demonstrated that patients with schizophrenia had significantly lower bilateral hippocampal volumes than patients with MDD. Taken together, these findings suggest that patients with schizophrenia have more severe reductions in hippocampal volume than patients with bipolar disorder and MDD.
Our correlation analysis did not find a significant correlation between hippocampal volume and illness duration in patients with schizophrenia; this finding was not totally consistent with those of previous studies. For example, one study found that smaller whole hippocampal volume was associated with longer duration of untreated psychosis.27 Another compared 2 independent cohorts with mean illness durations of 7 and 18 years; it revealed that patients with a shorter duration of illness had significant cross-sectional volume deficits only in the CA1 subfield, and more chronic schizophrenia patients showed diffuse cross-sectional volume deficits across all subfields.28 However, another study showed progressive hippocampal volume loss only in the early course of illness in patients with schizophrenia — not in the more chronic stages of illness — and higher exposure to atypical antipsychotic medication was related to a smaller decrease in hippocampal volume over time.29 A meta-analysis of 44 imaging studies showed that patients with first-episode and chronic schizophrenia had hippocampal volume reductions of similar size.30
To further clarify this issue, we conducted an additional analysis that divided our patients into 4 groups according to duration of illness (2.8 ± 2.0, 9.0 ± 1.3, 15.0 ± 2.2 and 26.4 ± 5.1 yr, separately) and found similar hippocampal volume deficits regardless of quite distinct illness durations ( Appendix 1, Table S3). The fact that all patients with schizophrenia in the present study used atypical antipsychotics chronically, and that we did not analyze hippocampal subfields, may have contributed to the discrepancy between our findings and those of previous investigations.
The pallidum, a major component of the basal ganglia, receives substantial γ-aminobutyric acid (GABA)–ergic inputs from the striatum (putamen and caudate) and sends direct outputs to the thalamus. Increased pallidal volumes and early-onset psychosis with short illness duration25 have been consistently demonstrated in previous MRI studies of schizophrenia.7,31 One potential mechanism for the enlargement of the pallidum is high blood flow in the striatal structures in schizophrenia,32 which may be caused by a hyperdopaminergic state.33,34 Antipsychotic use may play a vital role in this, because pallidal volume has been positively correlated with antipsychotic dose administered in schizophrenia groups;31,35 however, a larger pallidum volume has also been reported in unmedicated, healthy relatives of patients with schizophrenia,36 and individuals with an at-risk mental state.13 These findings suggest that the increased pallidal volume is related to a general vulnerability to psychopathology.
Studies have demonstrated a lower pallidum volume in patients with bipolar disorder than in those with MDD.37,38 Although the volume of the pallidum in patients with MDD has been less studied, a meta-analysis revealed a trend of a lower volume in these patients.24 Another study found that atrophy level in the left pallidum was positively correlated with the severity of suicidal risk in patients with MDD who had suicidal ideation.39 In summary, the findings of the present study indicate that changes in pallidal volume occur in different directions in schizophrenia and bipolar disorder or MDD; in this way, the pallidum serves as the subcortical structure with the most distinct volumetric features among the 3 disorders.
Limitations
This study had several limitations. First, participants in all of our patient groups were taking psychotropic medications, which can affect the basal ganglion–related structures of the putamen, caudate and pallidum. A cross-sectional meta-analysis reported that daily antipsychotic doses were positively correlated with the left pallidal volume and negatively correlated with right hippocampal volume.40 Another meta-analysis reported that higher antipsychotic exposure was significantly associated with an increased basal ganglia volume.41 However, a meta-analysis of longitudinal studies demonstrated no significant effect of antipsychotic treatment on caudate volume in schizophrenia.42 Still another meta-analysis7 indicated that many unmedicated patients demonstrated more severe deficits in hippocampal volume, indicating a normalization effect of antipsychotics on the hippocampus. Although the effects of antipsychotics on subcortical volumes are not totally consistent, they were likely the major confounders in this study.
Second, because of the cross-sectional design of our study, we could not determine whether these abnormalities developed gradually during illness, appeared before illness, or appeared in the early stages of illness. A meta-analysis of VBM studies revealed considerable overlap in the regions affected in both first-episode and chronic schizophrenia, including grey matter decreases in the thalamus, left uncus or amygdala region, left and right insula, anterior cingulate, and left inferior frontal gyrus.43 Another study in first-episode schizophrenia demonstrated significantly smaller volumes in the amygdala, hippocampus and thalamus, as well as in total cortical grey matter, in patients with schizophrenia compared to controls.44 A large-scale study of early-onset psychosis with a short illness duration (1.5 yr) found significantly lower hippocampal volumes and higher caudate and pallidal volumes in patients compared to controls.25 Together, these findings suggest that such abnormalities occurred in the early stages of the illness. Additional longitudinal follow-up studies of first-episode patients should be performed to examine progressive changes in these structures.
Third, the MRI images used in this study were collected between 2010 and 2019, and updates of console software took place each year during this period. Although the major purpose of these updates was to fix bugs in previous versions and make machine operation more smooth without a substantial effect on image properties, this was a potential confounder in the present study and should be considered in the interpretation of our findings.
Finally, we were unable to match patients with MDD with the other 2 diagnostic groups in terms of sex and illness duration because the MDD group had a higher number of women and a later onset of illness than the schizophrenia and bipolar disorder groups. Our findings related to the hippocampus should be interpreted with caution because Schmaal and colleagues10 reported a significant effect of onset age and illness duration on the hippocampal volume reductions in patients with MDD.
Conclusion
We used a large, single-site data set to identify common and distinct subcortical volumetric abnormalities in patients with schizophrenia, bipolar disorder and MDD. Our findings revealed that decreased thalamic volume is a common feature of these 3 major psychiatric disorders. The distinct volumetric differences we found in the pallidum and hippocampus for schizophrenia versus bipolar disorder or MDD may provide critical clues to a biological basis for the century-long Kraepelinian distinction between these illnesses.
Acknowledgements
The study was supported by grants from Taipei Veterans General Hospital (V109E-002-4[109]), Yen Tjing Ling Medical Foundation (CI109-02) and the Ministry of Science and Technology (99-2628-B-010-021-MY2, 102-2420-H-010-003, 103-2314-B-075-065-MY2, 104-2314-B-075-017, 105-2314-B-010-064-MY3, 108-2314-B-075-038 and 109-2314-B-075-062). The study also received technical support from the Big Data Center, Taipei Veterans General Hospital.
Footnotes
Competing interests: None declared.
Contributors: P.-C. Tu and W.-C. Chang designed the study. All authors acquired the data, which P.-C. Tu, W.-C. Chang and Y.-M. Bai analyzed. P.-C. Tu wrote the paper, which all authors reviewed. All authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
Data sharing: The data that support the findings of this study are available from the authors. Restrictions in relation to potentially person identifiable information apply.
- Received September 3, 2021.
- Revision received March 1, 2022.
- Revision received April 22, 2022.
- Revision received May 10, 2022.
- Accepted May 10, 2022.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.