
Abstract
Background: Borderline personality disorder (BPD) is characterized by a negative perception of others. Previous studies have revealed deficits and biases in facial emotion recognition. This study investigates the behavioural and electrophysiological correlates underlying facial emotion processing in individuals with BPD.
Methods: The present study was conducted between July 2012 and May 2014. In an emotion classification task, unmedicated female patients with BPD as well as healthy women had to classify faces displaying blends of anger and happiness while the electroencephalogram was recorded. We analyzed visual event-related potentials (ERPs) reflecting early (P100), structural (N170) and categorical (P300) facial processing in addition to behavioural responses.
Results: We included 36 women with BPD and 29 controls in our analysis. Patients with BPD were more likely than controls to classify predominantly happy faces as angry. Independent of facial emotion, women with BPD showed enhanced early occipital P100 amplitudes. Additionally, temporo-occipital N170 amplitudes were reduced at right hemispherical electrode sites. Centroparietal P300 amplitudes were reduced particularly for predominantly happy faces and increased for highly angry faces in women with BPD, whereas in healthy volunteers this component was modulated by both angry and happy facial affect.
Limitations: Our sample included only women, and no clinical control group was investigated.
Conclusion: Our findings suggest reduced thresholds for facial anger and deficits in the discrimination of facial happiness in individuals with BPD. This biased perception is associated with alterations in very early visual as well as deficient structural and categorical processing of faces. The current data could help to explain the negative perception of others that may be related to the patients’ impairments in interpersonal functioning.
Introduction
Patients with borderline personality disorder (BPD) have a biased and more negative perception of others. According to the DSM-5 model,1 this may impair their empathy and thus contribute to their interpersonal dysfunctioning (e.g., by triggering reactive, aggressive responses).2 There is increasing evidence for deficient or biased emotional face perception in individuals with BPD,3 which may contribute to the patients’ exaggerated anticipation of social threat and difficulties in social interactions.4 Patients with BPD are, for instance, more likely to judge others as being more negative and aggressive;5,6 to make more errors in facial emotion classification tasks, particularly regarding negative emotional expressions;7–9 and to ascribe negative emotions to neutral faces.5,10 According to other findings, patients with BPD may be regarded as emotionally hypersensitive for subtle facial cues, reflected by lower thresholds for emotion recognition in ambiguous or mixed emotional faces.11–13
Daros and colleagues3 have proposed a model according to which the increased arousal of patients with BPD may either lead to an enhanced detection of subtle facial threat or hinder the classification of intense facial emotions in binding attentional resources by salient social cues. This model may explain seemingly inconsistent results from various emotion recognition tasks. It is also congruent with neuroimaging studies that have revealed enhanced and prolonged amygdala activations,14,15 a decreased prefrontal inhibition of the amygdala and altered insular and anterior cingulate activations16–18 for emotional stimuli in patients with BPD. In combining eye tracking with functional MRI (fMRI), we recently found more and faster initial eye movements toward the eyes, and thus the most threatening part of angry faces, associated with increased amygdala activation in patients with BPD.14 In line with the assumption of an initial hypersensitivity for acute social threat, this may indicate alterations in very early stages of facial emotion processing. Nevertheless, little is known about the time course of facial emotion processing and its emotion-specific differences in individuals with BPD.
The electroencephalography-based event-related potential (ERP) technique provides a high temporal resolution allowing a noninvasive online registration of cortical processes.19 Emotional faces elicit a specific sequence of ERPs over time,20 starting with a very early positive wave, the P100, a component that is recorded at occipital sites about 100 ms after the presentation of any visual stimulus. The P100 is thus thought to reflect general primary visual analyses in the striate and extrastriate cortex that are not specific to (emotional) faces.21 This is followed by the N170, a negative wave recorded at temporo-occipital sites around 170 ms, which is thought to reflect the activation of face-specific neurons primarily in the fusiform gyrus or superior temporal sulcus with additional activation of a wider network, including the occipital cortex.22,23 The N170 may reflect the structural encoding of faces leading to the generation of a complete facial representation.24 Although these early components primarily reflect initial, visual (P100) and structural face (N170) processing that are mostly independent of the semantic stimulus content,25 there are also indications for modulatory influences of emotions that may be linked to stimulus saliency in terms of survival, reproduction and procreation arising from limbic input to the visual cortex.26–29 A later component, the P300, a positive wave that is recorded about 300–600 ms after stimulus onset at centroparietal sites, is particularly sensitive to psychological influences, such as anxiety, depression, alexithymia and aggression.30–33 The P300 is possibly generated in the extrastriate occipital inferior temporal and medial parietal cortices34 and has been linked to subsequent higher stages of emotional face processing and decisional processes implicated in working memory updating or conscious detection of change, cognitive closure or emotion categorization.
There is limited literature on the electrophysiology underlying facial emotion processing in individuals with BPD. A magnetoencephalographic (MEG) study35 revealed reduced M170 amplitudes, an N170 equivalent component, for faces displaying basic emotions, but also for neutral faces, houses and animals in patients with BPD compared with healthy individuals. This stimulus-independent reduction may reflect broad deficits in information processing at a relatively early perceptual level in individuals with BPD.35 Furthermore, several studies revealed reductions (for exceptions, see studies by Meares and colleagues36,37) in the P300 amplitude in patients with BPD compared with healthy volunteers (although not during emotion classification) in auditory oddball,38–40 go/no-go41 or Stroop tasks42 and after late feedback in a 2-choice reaction task.43 Taken together, previous results suggest alterations in early and later ERP components in individuals with BPD, but investigations of the time course of these alterations during an emotion classification task are missing.
Thus, the aim of the study was to investigate the behavioural and electrophysiological correlates underlying emotional face processing in individuals with BPD with a particular focus on the patients’ sensitivity for facial anger. We used a validated task12,44–47 with facial stimuli depicting blends of angry and happy expressions, thus containing emotionally ambiguous information. This design bears the potential to unravel interpretative biases evident in an increased proportion of anger judgments of such stimuli. In fact, we have previously found a specific interpretative bias or hypersensitivity for facial anger in patients with BPD in a task with faces displaying blends of different emotional expressions.12 In the present experiment, unmedicated female patients with BPD and healthy women had to classify facial emotions in a forced choice task while the electroencephalogram was recorded. The faces were preceded by task-irrelevant happily or angrily intonated sentences to increase the ecological validity of the task.46 We expected that, compared with healthy volunteers, patients would show reduced thresholds for anger recognition but also more misclassifications and prolonged response latencies for predominantly angry faces. As for the emotionally intonated auditory stimuli, we expected an increased influence of the angry intonation in patients, leading to an increased likelihood of classifying ambiguous faces as angry. We explored the ERPs underlying structural and categorical facial emotion processing, expecting a hyperresponsiveness for facial anger in patients with BPD compared with healthy volunteers.
Methods
Participants
We studied unmedicated women with a current DSM-IV diagnosis of BPD and healthy women who had never received a psychiatric diagnosis or undergone any psychological or psychiatric treatment. Participants were recruited through the resident’s registration office, advertisements and clinical referral from in- and outpatient units. Behavioural data were excluded in cases of positive toxicology screenings, brain damage or technical malfunctioning; EEG data were excluded if there was an insufficient number of trials owing to uncorrectable artifacts.
We verified handedness using the Edinburgh Handedness Inventory,48 and participants were required to have normal or corrected-to-normal visual acuity. General exclusion criteria were neurologic disorders, current alcohol/drug abuse (urine toxicology screenings) or alcohol/drug abuse in the last 2 months (interview), severe medical illness and use of psychotropic medication for at least 2 weeks before participation in the study. Additional exclusion criteria for patients were lifetime diagnosis of schizophrenia, schizoaffective or bipolar disorder and reported alcohol/drug dependence in the last 12 months. Only patients who currently fulfilled at least 5 DSM-IV criteria for BPD were included in the study.
The Ethics Committee of the Medical Faculty of the University of Heidelberg approved the study. All participants provided written informed consent after the study procedures were fully explained, and they were paid for their participation.
Measures
For each patient with BPD and control, the diagnostic process comprised an extensive telephone interview (about 45 min) to screen for inclusion/exclusion criteria followed by an onsite diagnostic appointment (about 3 h) involving structured clinical interviews (SCID-I;49 International Personality Disorder Examination50) to assess borderline diagnosis and axis I and II comorbidities as well as the Raven’s progressive matrices51 as an estimate for intelligence. All interviews were performed by experienced diagnosticians (masters in psychology or doctorate in medicine with several years of clinical training) who underwent standardized diagnostic training before the study. In addition, we assessed borderline symptom severity using the Borderline Symptom List (BSL52), state and trait anger using the State-Trait Anger Expression Inventory (STAXI,53 state, trait, reaction, anger-in, anger-out, anger-control subscales), emotional dysregulation using the Difficulties in Emotion Regulation Scale (DERS,54 acceptance, awareness, impulse, strategy, clarity, goals subscales) and depressiveness using the Beck Depression Inventory (BDI-II55).
Experimental protocol
After arrival in the laboratory, participants provided a urine sample for toxicology screening and filled in questionnaires. To perform the experimental task, they were seated in a sound-attenuated, dimly lit room with their heads restrained in a chin rest 1 m from a 21-inch computer screen and equipped with in-ear headphones. The electrode sites on the participants’ scalps and faces were cleaned and gently abraded before electrode placement. After a short training, participants completed 3 experimental runs of 15 min each (total participation time, including EEG preparation, training and short breaks between the runs was about 90 min).
Emotion classification paradigm
The emotion classification paradigm consisted of a previously validated12,45–47 forced-choice task in which participants had to classify faces depicting blends of angry and happy expressions by pressing a corresponding key for “angry” or “happy.” This task has been deemed suitable to detect an interpretative bias or hypersensitivity for facial anger in patients with BPD.12 Half of the faces within each emotional blend were preceded by a happily intonated sentence and half by an angrily intonated sentence with neutral content. These sentences were read by professional female and male actors and were validated in an independent sample before the experiment. Facial stimuli consisted of 2 male and 2 female faces56 that were morphed in 10% steps, resulting in a series of 7 pictures showing blends of the angry and happy expressions: predominantly happy faces (80:20%, 70:30%, 60:40% happiness:anger), maximally ambiguous faces (50:50% happiness:anger) and predominantly angry faces (40:60%, 30:70%, 20:80% happiness:anger). In total, the experiment comprised 840 trials presented in 3 experimental runs of 280 trials each in pseudorandomized order with no more than 3 presentations of the same emotional condition in a row. Each trial started with the presentation of a fixation cross and auditory presentation of an angrily or happily intonated sentence (2000 ms), a fixation cross without auditory stimulation (100 ms) followed by a facial stimulus (response-locked presentation, 1100 ms) and another fixation cross (450–650 ms).
Data acquisition and processing
The EEG was recorded with Ag/AgCl electrodes from 60 sites (equidistant reference system, Easy-Cap GmbH) using an average reference. Additionally, vertical and horizontal electro-oculograms (EOGs) were recorded from the epicanthus of each eye and from the supra- and infraorbital positions of the left eye. Electrode impedances were kept below 10 kΩ and signals were amplified with a 72-Kanal QuickAmp amplifier (Brain Products, GmbH). The pass-band was set to 0.01–200 Hz; the signals were digitized at 1000 Hz and stored to hard disk for later analysis. Data processing was conducted using Brain Vision Analyzer 2.0 (Brain Products, GmbH) and included renaming of EEG channels to a 10/20 system57 (small position deviations are marked with“′”), digital filtering (0.1–40 Hz, 24dB/octave roll-off), correction of eye-movement artifacts using an algorithm provided by Gratton and colleagues,58 semiautomatic rejection of trials with nonphysiologic artifacts, segmentation into 1300 ms periods (−100 ms to 1200 ms from stimulus onset) and baseline correction (reference: −100 ms to 0 ms from stimulus onset). Separate averages were computed for each electrode and combination of facial and auditory emotion at individual and group levels. Statistical analyses were conducted on ERP peaks for the P100 (maximum positive peak 80–130 ms at O1′, Oz, O2′) and N170 (maximum negative peak 130–230 ms at TP7′, TP8′, TP9′, TP10′, P7′, P8′, P9′, P10′, O1′, O2′, O9′, O10′) components and mean amplitude for the P300 (350–600 ms at Cz, CP1′, CP2′, CPz, CP3′ CP4′, P1′, Pz, P2′).
Statistical analysis
Behavioural data (proportion of anger classifications and response latencies) were subjected to analyses of variance (ANOVAs) using group (BPD, control) as a between-subjects factor and facial emotion (7 levels of anger–happiness intensity) and voice intonation (angry, happy) as within-subjects factors. We also ran analyses using multivariate ANOVA, which yielded similar results for the behavioural and ERP data in that all reported effects were significant using multivariate analyses except for the group × emotion interaction in the behavioural data, which reached only trend-level significance (p = 0.08). Hypothesis-driven univariate ANOVAs, however, revealed significant group differences in the proportion of anger classification for faces with 20% (p = 0.015) and 30% anger (p = 0.011) and in response latencies for faces with 20% anger (p = 0.028). Behavioural results remained stable after exclusion of 2 participants without reliable EEG data. We averaged across the sex of the faces because preliminary behavioural and ERP data analyses did not reveal any effect of sex (all p > 0.10). For the ERP data, separate ANOVAs had to be performed for the P100, N170 and P300 owing to the different localizations of these ERP components (see the data acquisition and processing section for the different sets of electrodes). Besides the factors group, facial emotion and voice intonation, analyses of P100 and N170 additionally comprised the within-subjects factor electrode site (P100: left, middle, right) and hemisphere (N170: left, right), respectively. Since response latencies were skewed, they were log-transformed before analysis. Where appropriate, we applied the Huynh–Feldt59 procedure to correct for potential violations of the sphericity assumption. All statistical analyses were 2-tailed, and we considered results to be significant at p < 0.05. In cases of significant effects, we used Dunn’s multiple comparison as post hoc tests, which include a Bonferoni correction for multiple testing. We additionally performed Pearson correlations to explore trade-off between accuracy (proportion of anger classification) and speed (response latencies) in the behavioural data and associations between behavioural and ERP data as well as self-reported traits. The results of these exploratory correlational analyses may be interpreted only descriptively owing to the limited power and the cumulation of type I errors.
Results
Participants
We recruited 36 unmedicated women with BPD (mean age 26.7 ± 6.0 [range 18–40] yr) and 29 healthy women (mean age 26.2 ± 6.0 [range 19–48] yr) for participation in the study. Behavioural data were excluded for 3 patients and 1 control (2 owing to positive toxicology screenings, 1 owing to organic brain damage and 1 owing technical malfunctioning), and EEG data were excluded for 1 patient and 1 control owing to uncorrectable artifacts. Thus, the results are based on the behavioural data of 33 patients and 28 controls and the EEG data of 32 patients and 27 controls. All participants were right-handed. Detailed demographic and psychometric information and group comparisons are provided in Table 1, and comorbid disorders of the patient group are presented in Table 2.
Demographic and psychometric data
Comorbidities of patients with borderline personality disorder
Behavioural results
Proportion of anger classification
Across diagnostic groups, participants generally classified predominantly angry faces (60%–80% anger) more often as angry and predominantly happy faces (20%–40% anger) as happy, while there was no general tendency for maximally ambiguous faces (main effect of facial emotion F6,354 = 973.55, p < 0.001, η2 = 0.94). Proportion of anger classification was also influenced by the auditory stimuli (main effect of voice intonation F1,59 = 27.86, p < 0.001, η2 = 0.32; interaction of voice intonation and facial emotion F6,354 = 5.68, p < 0.001, η2 = 0.09). Post hoc analyses showed that the voice intonation particularly influenced the rating of faces with 40%–60% anger (all p < 0.01). For instance, when an angrily intonated sentence preceded such a face, participants rated this face more often as angry.
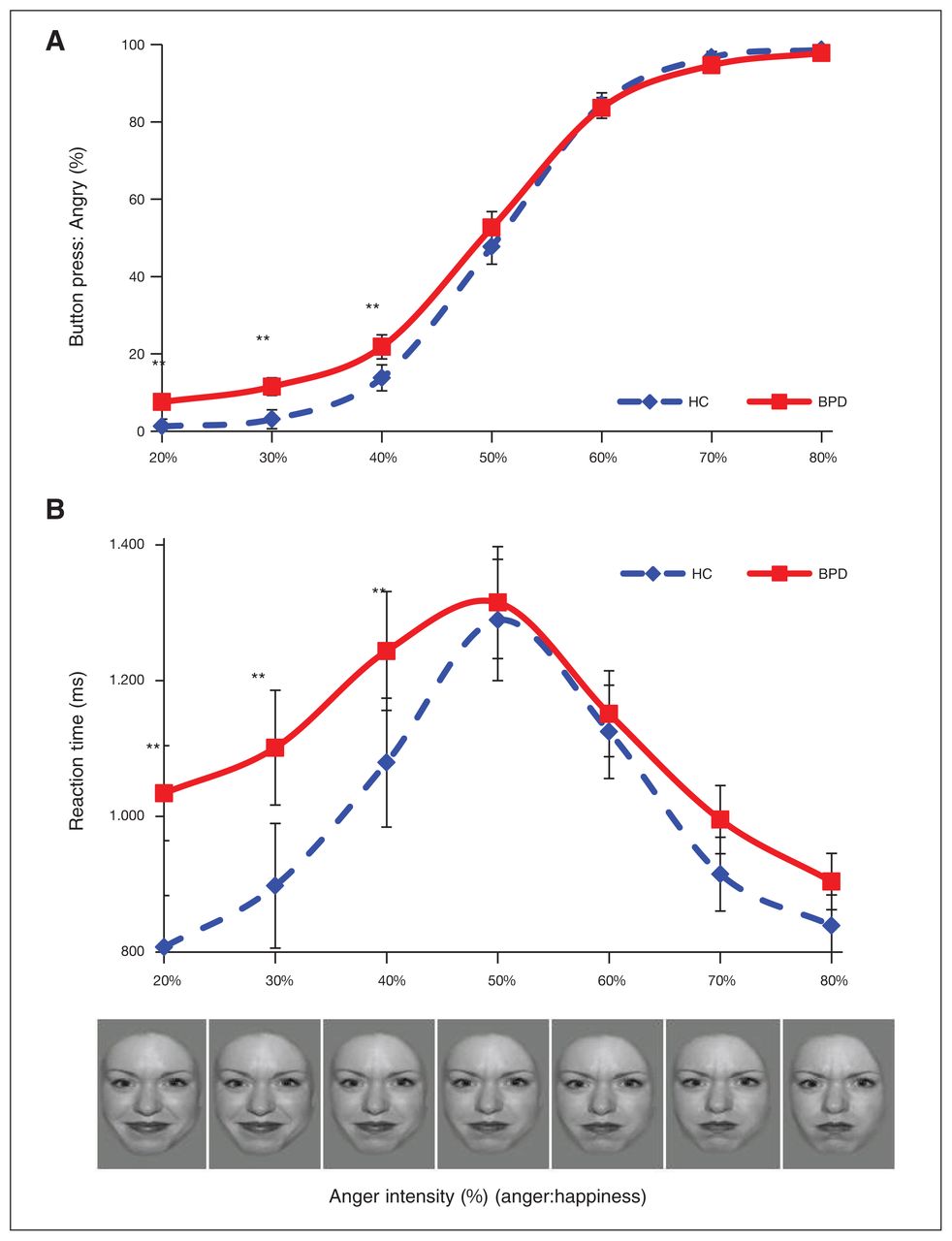
The ANOVA also revealed a significant group × facial emotion interaction (F6,354 = 2.89, p = 0.049, η2 = 0.05). According to post hoc tests, patients with BPD classified predominantly happy faces (20%–40% anger) more often as angry than controls (p < 0.01) and tended to misclassify predominantly angry faces (60%–80% anger) as happy (p > 0.05, Fig. 1A). There was no significant group × voice intonation interaction (p = 0.21).

(A) Mean proportion of anger classification in percent (± 1 standard error). (B) Mean response latencies in milliseconds (± 1 standard error) of patients with borderline personality disorder (BPD) and healthy controls (HC) averaged across auditory stimulus conditions. The X axis shows percentage of facial anger. **p < 0.01, *p < 0.05.
Response latency
Overall, participants responded faster for the less ambiguous faces and slower as faces turned ambiguous (main effect of facial emotion F6,354 = 55.78, p < 0.001, η2 = 0.49). The emotional voice intonation also had a significant effect: across groups, participants showed faster responses to predominantly happy faces (20%–40% anger) that were preceded by a happily intonated voice and to predominantly angry faces (60%–80% anger) preceded by an angry voice compared with predominantly happy faces (20%–40% anger) preceded by angry voices and predominantly angry faces (60%–80% anger) preceded by happy voices (interaction of voice intonation × facial emotion F6,354 = 2.58, p = 0.023, η2 = 0.04).
According to a significant group × facial emotion interaction (F6,354 = 3.00, p = 0.047, η2 = 0.05, Fig. 1B), patients with BPD responded slower than healthy volunteers, especially for predominantly happy faces (20%–40% anger, p < 0.01). There was no significant group × voice intonation interaction (p = 0.64).
As there were no significant interactions of group × voice intonation in the behavioural data (all p > 0.20) and no indications of such an effect in the ERP data (all p > 0.10 for mean amplitudes), the factor voice intonation was dropped from the analyses of the ERP data.
ERP results
P100
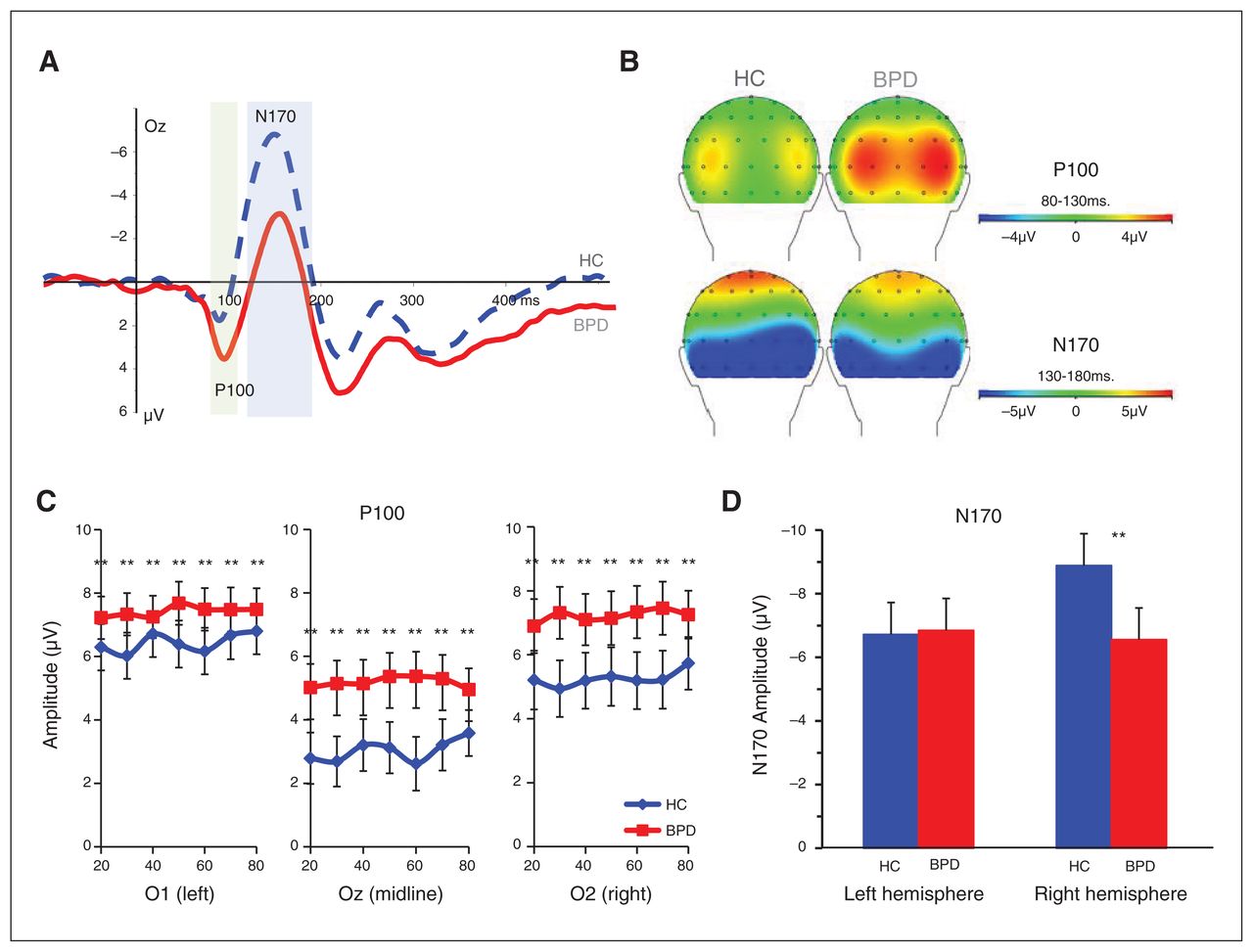
Across groups, P100 peak amplitudes were generally larger at lateral (O1′and O2′) than midline (Oz) electrode sites (main effect of electrode F2,114 = 40.89, p < 0.001, η2 = 0.42, ɛ = 0.93).
In addition, the ANOVA revealed a trend-level significant main effect of group (F1,57 = 2.83, p = 0.10, η2 = 0.05) and a significant group × facial emotion × electrode interaction (F12,684 = 1.91, p = 0.042, η2 = 0.03, ɛ = 0.83; Fig. 2A and B). Post hoc tests showed that the P100 was lateralized in healthy volunteers, with enhanced left hemispheric amplitudes (O1′ compared with Oz and O2′; anger intensities all p < 0.01), while patients with BPD did not show this lateralization effect (all p > 0.05 except for 50% anger: p < 0.01; Fig. 2C). Moreover, in healthy volunteers, the P100 amplitude was modulated by facial emotion. They had increased peaks for faces displaying 80% anger compared with faces displaying 20% anger (p < 0.01 for all electrodes), while patients with BPD showed enhanced P100 amplitudes independent of facial emotion (all p > 0.10).
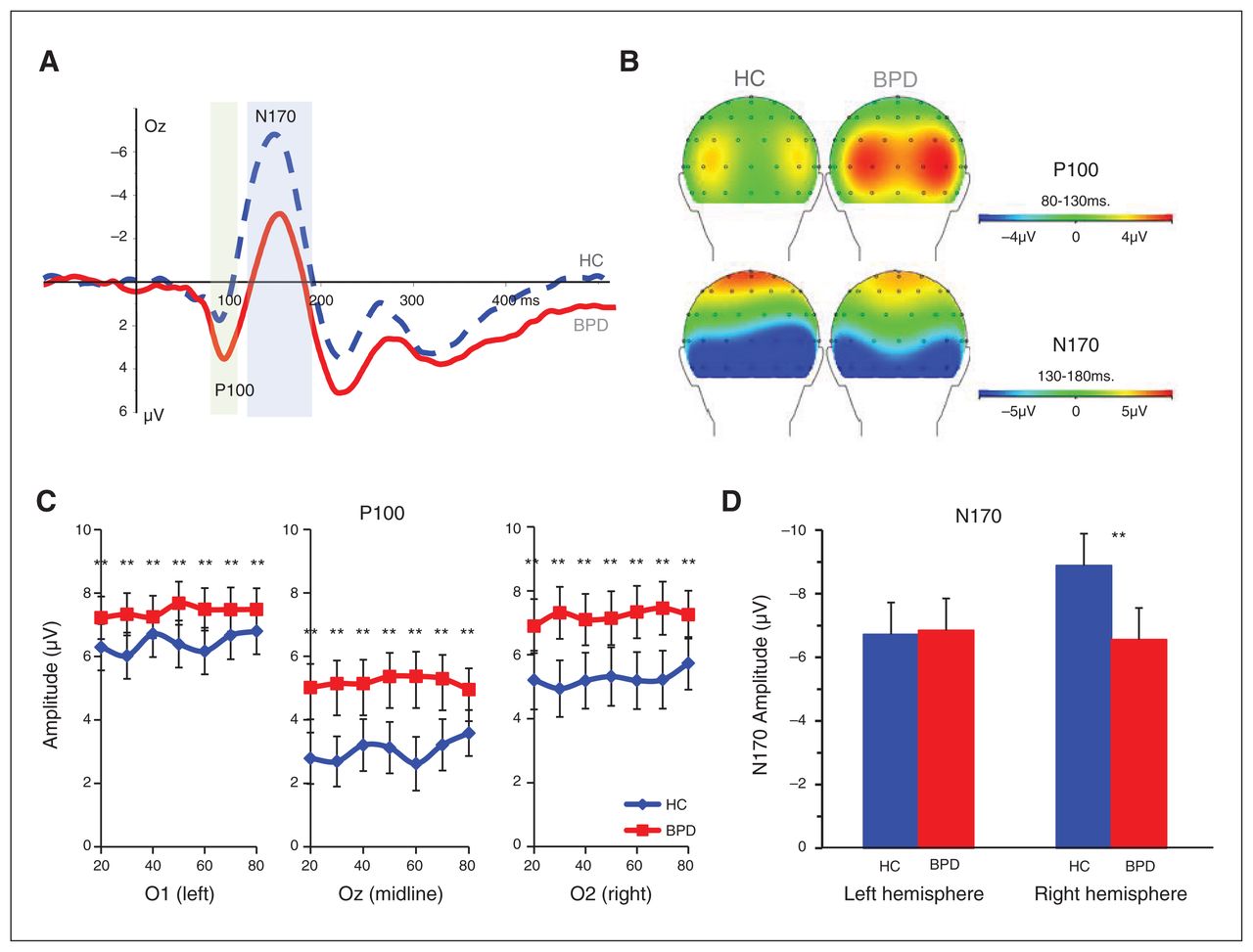
(A) Mean event-related potential (ERP) at Oz electrode position in patients with borderline personality disorder (BPD) and healthy controls (HC) averaged across auditory stimulus conditions. (B) Head views of P100 and N170. (C) Peak amplitude of P100. (D) Peak amplitude of N170. **p < 0.01, *p < 0.05.
Across groups, P100 peak latency tended to be increased for maximally ambiguous faces (main effect of facial emotion F6,342 = 2.17, p = 0.06, η2 = 0.04, ɛ = 0.83) and was delayed at left compared with midline and right hemispheric electrodes (main effect of electrode F2,114 = 8.92, p < 0.001, η2 = 0.14, ɛ = 1.0).
According to a significant main effect of group (F1,57 = 4.17, p = 0.046, η2 = 0.07), P100 peaks were delayed in patients with BPD compared with healthy volunteers (100.4 ms v. 95.3 ms); however, neither facial emotion nor electrode significantly interacted with group (all p < 0.10).
N170
Across groups, N170 peak amplitudes were more pronounced at right hemispheric electrodes (main effect of hemisphere F1,57 = 7.89, p = 0.007, η2 = 0.12, ɛ = 1.0). N170 amplitudes were also modulated by facial emotion (main effect of facial emotion F6,342 = 4,48, p < 0.001, η2 = 0.07, ɛ = 1.0), with larger amplitudes for faces with 80% anger than faces displaying lower anger intensity (20%–70% anger, all p < 0.01).
In addition, there was a significant group × hemisphere interaction (F1,57 = 13.62, p = 0.001, η2 = 0.19, ɛ = 1.0) according to which the N170 lateralization was present only in healthy volunteers (p < 0.01) but not in patients with BPD (p > 0.05). Thus, compared with healthy volunteers, patients with BPD had reduced N170 peak amplitudes at right hemispheric electrodes (p < 0.01, Fig. 2D). There was no significant interaction of group × facial emotion (p = 0.20) or group × facial emotion × hemisphere (p = 0.64).
There were no significant main or interaction effects for N170 peak latency (all p > 0.10).
P300
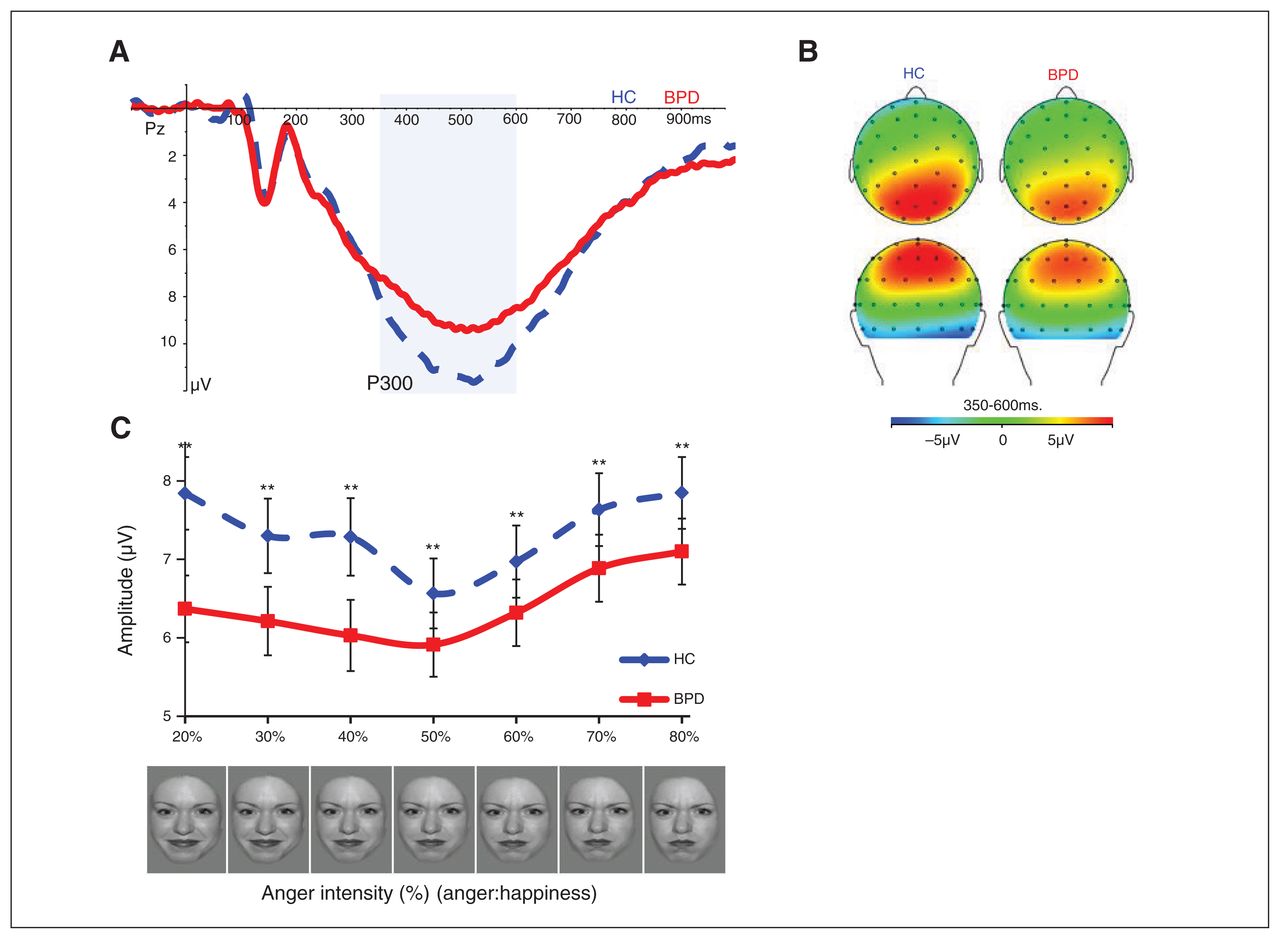
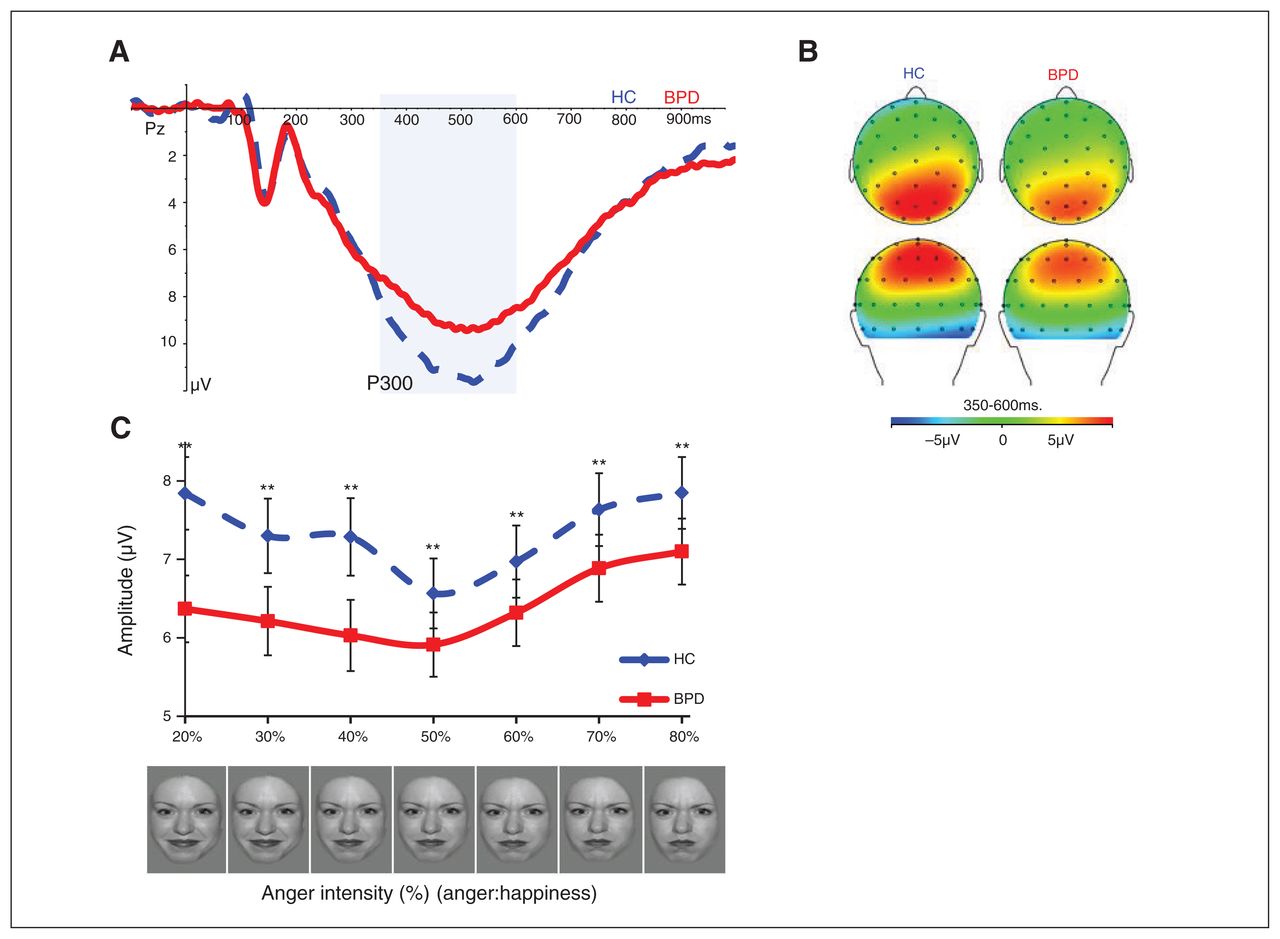
P300 amplitudes were largest for predominantly angry (60%–80% anger) or happy (20%–40% anger) faces and smallest for maximally ambiguous faces (50% anger, main effect of facial emotion F6,342 = 24.86, p < 0.001, η2 = 0.30, ɛ = 0.98).
According to a significant interaction of group × facial emotion (F6,342 = 3.72, p = 0.002, η2 = 0.06, ɛ = 0.98), P300 amplitudes were generally reduced in patients with BPD compared with healthy volunteers (all p < 0.01), with the strongest group differences for predominantly happy faces (20%–40% anger; Fig. 3). A closer inspection revealed that patients showed increased P300 amplitudes only for the most angry faces (70%–80% anger) compared with maximally ambiguous faces (50% anger, p < 0.01) as well as the most happy faces (20%–30% anger, p < 0.01). This strongly differed from the pattern found in healthy volunteers, whose P300 amplitudes were larger for both the most angry and happy faces compared with maximal ambiguous faces (all p < 0.01).
{kind=link}
{kind=link}
{kind=link}
(A) Mean event-related potential (ERP) at the Pz electrode position of patients with borderline personality disorder (BPD) and healthy controls (HC) averaged across auditory stimulus conditions. (B) Head views and (C) mean amplitude of P300. *p < 0.05; **p < 0.01.
Correlations
In both groups, response latencies and proportion of anger classification were positively correlated for predominantly happy faces (BPD: r31 ≥ 0.61, p ≤ 0.001; control: r27 ≥ 0.40, p ≤ 0.040); participants who responded slowest also classified predominantly happy faces more often as angry. In patients with BPD, anger classification and response latencies for predominantly happy faces were positively associated with N170 amplitudes (20%–40% anger: r30 ≥ 0.32, p ≤ 0.08), and response latencies for ambiguous and predominantly angry faces were negatively associated with P300 amplitudes (50%–80% anger: r30 ≥ −0.37, p ≤ 0.039). In controls, there were no correlations between behavioural and ERP data (r26 ≤ 0.30, p ≥ 0.10). In both groups, P100 and N170 amplitudes were positively associated (BPD: right hemispheric electrode for 20%–50% anger r30 ≥ 0.33, p ≤ 0.06; control: right and left hemispheric electrodes for 20%–80% anger r26 ≥ 0.40, p ≤ 0.038), with smaller (less negative) N170 amplitudes in those participants with greater (more positive) P100 amplitudes. In healthy volunteers, N170 and P300 amplitudes were positively correlated for predominantly happy and ambiguous faces (r26 ≥ 0.33, p ≤ 0.038). No correlations were found between N170 and P300 amplitudes in patients with BPD and between P100 and P300 amplitudes in both groups (r < 0.30, all p > 0.10).
We additionally found positive correlations between proportion of anger classification and the DERS emotional awareness subscale (30%–70% anger: r31 ≥ 0.34, p ≤ 0.06), BSL borderline symptom severity (20%–60% anger: r30 ≥ 0.31, p ≤ 0.09) and BDI depressiveness (40%–60% anger: r30 ≥ 0.32, p ≤ 0.09) in patients with BPD but not in healthy volunteers (r27 ≤ 0.30, p ≥ 0.10). In patients with BPD, P100 amplitudes were positively correlated with DERS emotional awareness (20%–80% anger: r30 ≥ 0.33, p ≤ 0.07; no associations in controls: r27 ≤ 0.30, p ≥ 0.10), while P300 amplitudes were positively related with anger suppression (STAXI anger-in; 20%–80% anger: r30 ≥ 0.40, p ≤ 0.024; no associations in controls: r27 ≤ 0.30, p ≥ 0.10).
Comorbid psychiatric disorders
As influences of depression, posttraumatic stress disorder (PTSD) and social anxiety on emotional faces processing have been previously reported, we compared patients with BPD with and without depressive disorder (current diagnosis of major depression or dysthymia), current PTSD and current social anxiety disorders (current diagnosis of social phobia or avoidant personality disorder) in additional group × emotional facial expression ANOVAs. These analyses revealed no significant main effect of group or group × facial expression interaction for depression (n = 10 with and n = 32 without current depressive disorder), PTSD (n = 12 with and n = 21 without current PTSD) and social anxiety (n = 14 with and n = 18 without current social anxiety disorder) for behavioural and ERP data (all p > 0.05).
Discussion
To our knowledge, this is the first study to investigate temporal dynamics of facial emotion processing in patients with BPD using an EEG ERP technique with a particular focus on the patients’ sensitivity to facial anger. The results confirm alterations or biases in very early stages of face processing, as has been hypothesized on the basis of eye-tracking and neuroimaging studies.14–16 In addition to these early alterations, patients with BPD showed deficiencies in further stages of structural and categorical face processing that may be related to previously reported deficits in emotion classification, supporting a recent model on altered facial classification.3
The present study revealed an enhanced likelihood to misclassify predominantly happy faces (20%–40% anger) as angry in patients with BPD. This is consistent to previous results revealing a specific bias for anger in a similar task with faces displaying blends of all 6 basic emotions12 and may thus indicate an increased sensitivity or lower threshold for subtle cues of social threat. This is in line with increased reflexive gaze orientation toward threatening facial cues.14 Further indications for such a hypersensitivity were also found in neuroimaging studies that revealed enhanced and prolonged amygdala activations and a decreased prefrontal inhibition of amygdala for emotional faces and socially threatening stimuli in patients with BPD.14–16 In the present study, a higher proportion of anger classification was found in patients with increased levels of self-reported unawareness of their own emotions. In addition, misclassification of predominantly happy faces (20%–40% anger) as angry was related to the severity of borderline symptomatology, whereas classification of more ambiguous faces (40%–60% anger) as angry was related to depressiveness. These exploratory correlational results support the alternative DSM-5 model of BPD claiming a more negative perception of others that might underlie the patients’ impairments in interpersonal functioning.1 Importantly, the present results may also indicate deficits in the classification of positive facial emotions, such as happiness, in patients with BPD. This is consistent with the results of a recent behavioural study60 that revealed both an earlier detection for anger and a slower recognition of facial happiness in patients with BPD using different intensities of happy, angry and fearful facial expressions. In line with the previously reported behavioural deficiencies in classifying faces displaying high intensities of negative and particularly angry expressions,3 patients in the present study also tended to classify predominantly angry faces (60%–80% anger) less accurately than controls. Based on the model proposed by Daros and colleagues3 in which misclassification of intense negative facial emotions are partially explained by a depletion of cognitive resources required to disengage attention from highly salient emotional stimuli, we expected longer response latencies specifically for the most angry faces (i.e., 80% anger). However, patients with BPD responded generally slower than healthy volunteers (20%–80% anger), and this effect was most pronounced for predominantly happy faces (20%–40% anger). The positive correlations between proportion of anger classification and response latencies suggests that the patients’ misclassifications did not result from a trade-off between accuracy and speed and thus do not reflect an impulsive response style. Importantly, subgroups of patients with BPD with and without a current diagnosis of depressive disorders, PTSD and social anxiety disorders, which are highly prevalent in individuals with BPD and have been previously associated with a hypervigilance for social threat cues61,62 and a reduced facial happiness recognition, did not significantly differ in the proportion of anger classification, response latencies and ERP data.
By adding emotionally intonated auditory stimuli, we could investigate the sensitivity for facial anger in a more ecologically valid setting.46 Contrary to our hypotheses and the previously reported deficits in multisensory integration of emotional information in patients with BPD,63 the emotionally intonated auditory stimuli affected the proportion of facial anger classification similarly in patients and healthy volunteers. Both groups showed faster responses in congruent trials of voice and facial emotion than in incongruent trials, and the voice had strongest effects on the classification of faces with 40%–60% anger. This result means that patients with BPD — comparable to healthy controls — are able to benefit from a second sensory channel in case the information is synergistic. Further research is required to investigate auditory/bimodal emotion processing in individuals with BPD.
Besides behavioural alterations, the present study revealed a pattern of changes in very early and intermediate stages of facial emotion processing in patients with BPD. Irrespective of facial emotion, patients showed increased P100 amplitudes, a component that reflects primary visual analyses in the striate and extrastriate cortex.21 Contrary to this, P100 amplitudes were modulated by facial emotion in healthy volunteers, with significantly greater amplitudes for highly angry (80% anger) faces than faces with 20%–70% anger. This pattern relates to previous reports of enhanced P100 amplitudes for negative compared with happy64 or neutral faces65 in healthy volunteers and may reflect increased limbic input to the visual cortex in the presence of social threat.26 Interestingly, enhanced P100 amplitudes for various emotional faces were previously reported in students with high social anxiety66 as well as in healthy volunteers after an experimental provocation of reactive aggression,67 indicating a trait- (social anxiety, BPD) and state-dependent (provocation) early hypervigilance in the visual cortex, which may increase the attention for incoming social information. The enhanced P100 amplitudes of patients with BPD in the present study could thus reflect the patients’ general hyperresponsiveness for (potentially threatening) information, which, according to the alternative DSM-51 model of BPD, may, in association with a more negative perception of others, lead to impaired interpersonal functioning.
In addition to this early hyperresponsiveness, patients with BPD showed deficits in subsequent stages of emotional face processing, as reflected by reduced temporo-occiptal N170 and centroparietal P300 amplitudes. The N170, which reflects structural analyses of facial information, including the structural encoding of faces, in the fusiform face area and the superior temporal sulcus23 was lateralized in healthy volunteers. This lateralization is in agreement with the hypothesis of a preferential involvement of the right hemisphere in configurational facial analysis that has been confirmed by increased right posterior–inferior temporal N170 amplitudes for facial stimuli in previous ERP studies.25,68 Patients with BPD had significantly reduced right hemispheric N170 amplitudes and thus no right-lateralization. Comparably, Merkl and colleagues35 reported decreased temporo-occipital M170 amplitudes for facial stimuli in patients with BPD compared with healthy volunteers. Positive correlations between P100 and N170 amplitudes suggest a cascade effect with strongest deficits in structural processing and encoding of faces in patients with the largest initial visual hyperreponsiveness, which might explain the patients’ face classification impairments.
Patients with BPD also had reduced centroparietal P300 amplitudes. This component is thought to reflect higher stages of emotional face processing, including emotional categorization, working memory updating and cognitive closure processes that are highly sensitive to psychological influences. For instance, reduced P300 amplitudes in impulse control tasks have been reported in individuals with BPD41–43 and impulse control disorders or reactive aggression (for a review, see Patrick69) and have been interpreted as a correlate of the externalizing factor that these disorders have in common.69 Although the results of these tasks are difficult to compare with the present facial processing results, the general reductions in P300 amplitudes may partly reflect enhanced externalizing behaviour of patients with BPD. Supporting this assumption, we found the largest P300 amplitudes in patients who reported greatest withholding or suppression of anger. Additionally, the pattern of P300 alterations of patients also indicates deficits in attentive categorization of the emotional intensity. In line with the previously described P300 modulation by both pleasant and unpleasant stimuli,20 healthy participants showed increased amplitudes for both predominantly happy (20%–40% anger) and angry (60%–80% anger) compared with maximally ambiguous facial expressions (50% anger), while patients with BPD showed poorer discrimination between faces displaying 20%–60% anger and only enlarged P300 amplitudes for faces displaying 70%–80% anger. Similarly reduced P300 amplitudes for predominantly happy faces have been previously reported in depressive individuals,70 which may suggest an association with the patients’ negative perception of others and emotional negativity. Thus, the results indicate deficits in the processing and discrimination of facial happiness and a hypervigilance to full-blown expressions of anger, which could at least partially explain the deficits observed in the behavioural task.
Limitations
To our knowledge, this is the first study to examine the temporal dynamics of facial emotion processing in a large group of patients with BPD compared with age- and IQ-matched healthy women using an EEG-based ERP technique in an ecologically more valid setting. However, several limitations of the present study should be noted. First, we included only female patients with a number of comorbidities. Although this is in line with most of the previously published studies on emotional face processing in patients with BPD3 and reflects a typical pattern of comorbid psychiatric disorders,71 borderline-specific conclusions should be drawn with caution. We would therefore encourage studies that include clinical control groups, such as patients with major depression, social anxiety disorder or PTSD, as well as male participants. Second, further studies need to include self-reports and physiologic measures to assess arousal, alexithymia or empathy, which have been hypothesized to be important factors in explaining the alterations in emotional face processing in patients with BPD.3,72 Third, the temporal restrictions and the need of a large amount of trials owing to the small signal-to-noise ratio of the ERPs made us focus on facial anger and happiness and to not include a silent control condition. Therefore, we cannot rule out a general effect of auditory stimulation on information processing in patients with BPD. It remains unclear why the auditory stimulation did not have strong effects on the facial emotion processing in the present study, which is contrary to auditory modulation of early stages of face processing found in healthy individuals.73 It may be noted that auditory stimuli were presented before facial expression and were task-irrelevant, which may have reduced their impact on facial emotion processing.46 The present results therefore need to be regarded as a first attempt to investigate the time course of alterations in facial information processing in patients with BPD that raises further questions for future studies, including a more precise investigation of interactions between auditory and visual stimulation. Moreover, we cannot disentangle a specific bias for facial anger from an inability to recognize and discriminate happiness or a general tendency to misclassify emotions. Yet, our results are highly consistent to a previously reported lower threshold for facial anger in a study using various combinations of all 6 basic emotions without an auditory stimulation.12 Further studies are, however, needed to disentangle deficits in the processing and recognition of facial happiness from an anger hypersensitivity.
Conclusion
Our data indicate a very early hyperresponsiveness for emotional faces independent of the emotional intensity or its valence in patients with BPD and subsequent deficits in both structural and categorical emotional face processing (e.g., poorer discrimination of happy and emotionally ambiguous faces, but a hyperresponsiveness for highly angry faces). These electrophysiological findings may underline the behavioural findings of enhanced sensitivity for subtle cues of facial threat, deficits in the discrimination of facial happiness as well as deficits in the classification of highly socially threatening facial stimuli. Electrophysiological and behavioural alterations were strongest in patients with most negative affectivity and unawareness of own emotions. The ability to decode emotional information from facial expressions is important for the regulation of emotion and the fine graining of social responses. Different mechanisms, such as an enhanced sensitivity for facial anger or deficits in the recognition of positive facial information, may contribute to findings of a more negative perception of others in patients with BPD and may be a prerequisite for the patients’ impaired interpersonal functioning. The results can thus be regarded as a further step to understand the psychological and neurobiological underpinnings of BPD, which may help to improve psychotherapeutic strategies for the patients’ impairments in interpersonal functioning.
Acknowledgments
The authors thank K. Herwig for supporting the EEG measurement and analysis, L. Kramer, L. Müller, A. Gäbel and D. Gescher for their help with data collection, the Informatics team for programming, and the team of the Clinical Research Group on Mechanisms of Disturbed Emotion Processing in Borderline Personality Disorder (KFO 256) for participant recruitment and organization. The study was supported by grants from the German Research Foundation (DFG) awarded to S.C. Herpertz (He 2660/12-1; He 2660/7-2). Preliminary data of this study were presented at the DGPPN conference 2013 in Berlin and at the EPA Conference 2014 in Munich, Germany.
Footnotes
Competing interests: None declared.
Contributors: N. Izureta, R. Oelkers-Ax, M. Bohus, S. Herpertz and K. Bertsch designed the study. N. Izureta, K. Nagy, F. Mancke, M. Bohus and K. Bertsch acquired the data, which N. Izureta, R. Oelkers-Ax, S. Herpertz and K. Bertsch analyzed. N. Izureta and K. Bertsch wrote the article, which all authors reviewed and approved for publication.
- Received August 6, 2014.
- Revision received February 23, 2015.
- Accepted April 4, 2015.