
Abstract
Background: Treatment development that targets cognitive impairment is hampered by a lack of biomarkers that can predict treatment efficacy. Erythropoietin (EPO) improves verbal learning and memory in mood disorders, and this scales with an increase in left hippocampal volume. This study investigated whether pretreatment left hippocampal volume, interhemisphere hippocampal asymmetry or both influenced EPO treatment response with respect to verbal learning.
Methods: Data were available for 76 of 83 patients with mood disorders from our previous EPO trials (EPO = 37 patients; placebo = 39 patients). We performed cortical reconstruction and volumetric segmentation using FreeSurfer. We conducted multiple linear regression and logistic regression to assess the influence of left hippocampal volume and hippocampal asymmetry on EPO-related memory improvement, as reflected by change in Rey Auditory Verbal Learning Test total recall from baseline to post-treatment. We set up a corresponding exploratory general linear model in FreeSurfer to assess the influence of prefrontal cortex volume on verbal learning improvement, controlling for age, sex and total intracranial volume.
Results: At baseline, more rightward (left < right) hippocampal asymmetry — but not left hippocampal volume per se — was associated with greater effects of EPO versus placebo on verbal learning (p ≤ 0.05). Exploratory analysis indicated that a larger left precentral gyrus surface area was also associated with improvement of verbal learning in the EPO group compared to the placebo group (p = 0.002).
Limitations: This was a secondary analysis of our original EPO trials.
Conclusion: Rightward hippocampal asymmetry may convey a positive effect of EPO treatment efficacy on verbal learning.
Clinical trial registration: Clinicaltrials.gov NCT00916552.
Introduction
Mood disorders are among the top contributors to the global burden of disease.1 However, current treatment options are limited by insufficient efficacy for depressive symptoms in 30% to 40% of patients2 and substantial cognitive impairments in 30% to 60% of patients during periods of remission,3–5 for which there are no clinically available treatments.6–9 These limitations have led to great research interest in identifying neuroimaging and neurocognitive biomarkers that predict treatment efficacy for mood symptoms and cognition to aid in the development of more effective, personalized treatments.
A recent systematic review identified more than 50 studies of neuroimaging and neurocognitive biomarkers associated with efficacy on mood symptoms in patients with mood disorders.10 Larger prefrontal cortex (PFC) volume, greater white matter integrity and better cognitive performance at baseline have been consistently associated with greater treatment success, although smaller hippocampal volume may also be related to better response.10 These findings indicate that better “brain reserve” and cognitive function increase the chances of treatment success for mood symptoms. Notably, only 2 studies have examined baseline biomarkers associated with efficacy related to cognition.10 These studies were based on data from our randomized controlled trials investigating the effects of 8 weekly infusions of the multifunctional growth hormone erythropoietin (EPO) in mood disorders.11,12 Both reports documented positive associations between baseline cognitive impairment on neuropsychological tests and patients’ chances of achieving treatment efficacy with respect to verbal learning and global cognition, respectively.13,14 However, no study has investigated pretreatment neuroimaging measures associated with treatment efficacy for cognition in mood disorders. This lack of insight into neuroimaging predictors of cognitive improvement was highlighted by the International Society of Bipolar Disorders Targeting Cognition Task Force as a key methodological impediment for progress in the development of new cognition treatments.15 Specifically, insight into the neurocircuitry targets for cognition treatments has the potential to aid patient stratification for cognition trials, which again could increase signal detection, minimize the unnecessary exposure of patients to novel investigational treatments, and shorten the time to bring novel cognition treatments to patients.
The hippocampus is a promising treatment target and neuroimaging biomarker for predicting efficacy related to cognition because of illness-associated hippocampal volume reductions across affective and psychotic disorders.16,17 Specifically, MRI and postmortem immunohistochemical studies of patients with mood disorders have revealed a reduction in overall hippocampal volume18,19 and shrinkage of hippocampal subregions.20–23 Such hippocampal shrinkage may result from dendritic retraction, pyramidal cell death and suppression of neurogenesis due to glucocorticoid overexposure24–26 — deficits in plasticity that have a negative effect on hippocampus-dependent memory.27 Conversely, there is consistent evidence for an association between hippocampal volume increase and cognitive improvements across affective and psychotic disorders following treatment with EPO, lithium or aerobic exercise.28 In particular, we have found that EPO-associated improvement of verbal learning in patients with mood disorders was accompanied by — and correlated with — increased subregional left hippocampus volume.29 Hippocampal volume change may thus be a common biomarker of cognitive impairment and cognitive improvement in mood disorders. Further, loss of interhemisphere hippocampal asymmetry has emerged as a putative biomarker of cognitive decline in neurologic and neuropsychiatric conditions. In healthy individuals, the right hippocampus tends to be larger than the left,30 whereas patients with mild cognitive impairment show little hemispheric hippocampal asymmetry31,32 and patients with type 2 diabetes or Alzheimer disease show the opposite pattern of asymmetry.32,33 Rightward (left < right) hippocampal asymmetry may thus be a marker of “brain reserve” and a possible predictor of patients’ chances of treatment efficacy related to cognition.
This report is based on data from our EPO trials in patients with bipolar disorder or treatment-resistant unipolar depression.11,12 In this report, we addressed the following question: Do pretreatment left hippocampal volume and/or left–right hippocampal asymmetry influence EPO treatment response for verbal learning? We hypothesized that EPO-related verbal memory improvement would be predicted by smaller left hippocampal volume and/or left < right hippocampal asymmetry. For exploratory purposes, we also examined whether verbal memory improvement was predicted by larger pretreatment PFC volume. Our findings may help elucidate neuroimaging-based measures that predict treatment efficacy for cognition and can guide future personalized treatments targeting cognitive impairments.
Methods
Study participants
A description of the 2 randomized, double-blind, placebo-controlled EPO trials can be found elsewhere.11,12 In brief, trial participants were recruited between September 2009 and October 2012 through the Copenhagen Clinic for Affective Disorders and advertisements on relevant websites. Participants were screened using the Schedules for Clinical Assessment in Neuropsychiatry.34 Included participants had an ICD-10 diagnosis of unipolar disorder that met the criteria for treatment resistance based on the Treatment Response to Antidepressant Outcome35 with moderate depression (Hamilton Depression Rating Scale 17-item [HDRS-17]36 score ≥ 17) or bipolar disorder in partial remission (HDRS-17 and Young Mania Rating Scale37 scores ≤ 14) with subjective cognitive problems. There were no differences between the EPO- or placebo-treated participants in terms of diagnosis, symptoms, age, sex, education or illness load.11,12
Procedures
Patients were randomized to receive 8 weekly intravenous infusions of EPO (Eprex; 40 000 IU; Janssen-Cilag) or saline (NaCl 0.9%; placebo) as an add-on to their antidepressant or mood-stabilizing treatment in a double-blind manner. Blood tests and blood pressure were taken weekly during the trial, and the examiners were blind to the results. Screening, blinding procedures and safety precautions are reported elsewhere.11,12 Cognition was assessed at weeks 1 (baseline), 9 (1 week after treatment completion) and 14 (6-week follow-up) using a neuropsychological test battery that included the Rey Auditory Verbal Learning Test (RAVLT).11,12 Change in verbal learning indexed by RAVLT total recall from weeks 1 to 9 was the primary end point in the bipolar disorder study and a tertiary outcome in the unipolar disorder study (mood symptoms were primary and secondary end points). Three equivalent alternate versions of the RAVLT were administered at weeks 1, 9 and 14 in a counterbalanced fashion to limit learning effects. Mood symptoms were assessed using the HRDS-17, Beck Depression Inventory38 and Young Mania Rating Scale37 at weeks 1, 5, 9 and 14. Whole-brain MRI was performed at weeks 1 and 14.
Patients and outcome assessors were blinded to treatment allocation throughout the study and data analysis. The trial was carried out in accordance with the latest version of the Declaration of Helsinki; was approved by the local ethics committee, Danish Medicines Agency and Danish Data Agency; and was registered at clinicaltrials.gov (no. NCT00916552). After a complete description of the study, written informed consent was obtained from all participants.
MRI protocol
Whole-brain structural MRI data were obtained from all participants at the Danish Research Centre for Magnetic Resonance at baseline. The MRI scans were performed on a 3T Siemens Trio MR scanner with an 8-channel head array coil and using a high-resolution 3D T1-weighted spin echo protocol with the following parameters: inversion time 800 ms, echo time 3.93 ms, repetition time 1540 ms, flip angle 9°, field of view 256 × 256, 192 slices.
Structural data processing
We performed cortical reconstruction and volumetric segmentation using the FreeSurfer image analysis suite version 6.0.0 (http://surfer.nmr.mgh.harvard.edu/). The technical details have been previously described.39 Briefly, the image analysis pipeline included correction for intensity homogeneity, motion correction, removal of nonbrain tissue, segmentation of the subcortical white matter and deep grey matter volumetric structures (including the hippocampus, amygdala, caudate, putamen and ventricles), intensity normalization, tessellation of the grey matter/white matter boundary, and automated topology correction and surface deformation following intensity gradients to optimally place the grey/white and grey/cerebrospinal fluid borders at the location where the greatest shift in intensity defines the transition to the other tissue class. The resulting cortical models were registered to a spherical atlas based on individual cortical folding patterns to match cortical geometry across participants. Automated cortical parcellation was performed using the Desikan–Killiany Atlas,40 which labels 34 cortical parcellations in each hemisphere with respect to gyral and sulcal structure. Finally, several surface-based data were created, including representations of cortical surface area, volume and thickness.41 The volumetric segmentations and cortical reconstructions were visually inspected for accuracy, and larger errors in the reconstruction of the pial surfaces were corrected.
Regions of interest
Based on our a priori hypotheses, we used the FreeSurfer automated volumetric segmentation of the left and right hippocampi as regions of interest in the statistical analysis of the impact of baseline left hippocampal volume and hippocampal asymmetry on treatment response to EPO on verbal memory. For the exploratory surface-based analysis, we initially restricted the search volume to the PFC. Left and right hemisphere PFC masks were therefore constructed by adding the superior frontal, rostral and caudal middle frontal, pars opercularis, pars triangularis, pars orbitalis, lateral and medial orbitofrontal, precentral and frontal pole regions from the automated cortical parcellation according to the Desikan–Killiany Atlas described above.40
End point
Treatment response to EPO related to verbal learning was defined as change in RAVLT total learning scores from weeks 1 to 9 (baseline to treatment completion).
Predictors
The predictor variables included in our analysis of whether left hippocampal volume influenced EPO treatment response on verbal learning were as follows: treatment (EPO, placebo), left hippocampal volume, the interaction between treatment and left hippocampal volume, right hippocampal volume, total intracranial volume (TIV), age and sex.
The predictor variables included in our analysis of whether rightward hippocampal asymmetry influenced EPO treatment response on verbal learning were as follows: treatment, hippocampal asymmetry, the interaction between treatment and hippocampal asymmetry, total hippocampal volume (left and right), TIV, age and sex.
We did not include diagnosis in the above models, because we had previously found no effect of diagnosis on the cognitive benefits of EPO treatment.14 For significant associations, we added pretreatment depression severity (HDRS-17 score), number of concomitant medications and whether patients received lithium (yes/no) as covariates to explore the potential role of these clinical variables.
We calculated the Hippocampus Asymmetry Index (HAI) for each participant using the following formula: HAI = ([right hippocampal volume − left hippocampal volume] / total hippocampal volume) × 100% (see Yue and colleagues32 and Milne and colleagues42).
Statistical analysis
Hippocampal volumetric analysis
We implemented multiple linear regression to associate left hippocampal volume and HAI with change from baseline to post-treatment in verbal learning (on a continuous scale). All analyses were conducted in SPSS, version 22.0 (SPSS Inc.).
Surface-based analysis
To address the question of whether there are regional differences in cortical thickness, surface area or volume in the PFC at baseline that could influence EPO treatment response on the RAVLT, we set up a linear model in FreeSurfer and restricted the search volume to the PFC region of interest. We examined the association between the 3 cortical representations and baseline-to-follow-up changes in verbal memory (continuous scale). The statistical models included a treatment factor (EPO v. placebo) and participants’ changes in verbal memory scores and were adjusted for age, sex and estimated TIV. However, the model for cortical thickness excluded the TIV regressor because of a lack of statistically significant associations between TIV and cortical thickness.43 We computed 2 contrasts: the average effect of baseline-to-follow-up change in verbal memory regressing out the effect of treatment group, and the interaction effect between changes in verbal memory scores and treatment. For exploratory purposes, we repeated the analyses extending the search volume to the entire cortex. We assessed the statistical significance of the analyses using permutation-based cluster-wise correction for multiple comparisons using a vertex-wise cluster-forming threshold p < 0.0001.44 We further corrected the p values, running the surface-based models separately for the 2 hemispheres. Clusters were considered significant at a corrected p < 0.05.
Results
Patient flow and characteristics
Table 1 displays the characteristics of the EPO- and placebo-treated patients with structural MRI data at baseline. Of the 84 patients randomized to EPO (n = 42) or saline (n = 42), 1 patient (EPO) withdrew at baseline, and 1 (placebo) chose to terminate the trial in week 5. The RAVLT data were missing for 2 patients (1 EPO, 1 placebo). Data were lost because of technical problems/artifacts for 4 participants (3 EPO, 1 placebo). Therefore, baseline MRI data were available and analyzed for 76 of the 83 (92%) randomized patients from the trials (EPO = 37, placebo = 39). The EPO and placebo groups were well balanced for demographic and clinical variables. At baseline, the EPO group had smaller HAI than the placebo group (mean ± SD = 1.2 ± 2.0 v. 2.3 ± 2.0, respectively). The EPO-treated patients displayed a greater improvement in verbal memory than the placebo-treated patients (4.5 ± 7.6 v. 1.2 ± 5.8, respectively; t74 = 2.16; p = 0.034). Twenty-one (57%) EPO-treated patients and 6 (15%) placebo-treated patients displayed a clinically relevant verbal memory improvement (p < 0.0001, Fisher exact test).
Participant characteristics
Hippocampal volumetric analysis
Does left hippocampal volume at baseline influence EPO treatment response for verbal memory?
Left hippocampal volume did not significantly influence the effect of EPO on verbal memory (p = 0.51; Table 2). However, we did find a main effect of right hippocampal volume on nonspecific verbal memory change from baseline to post-treatment (p = 0.019). For every cubic millimetre increase in right hippocampal volume, we found a 1.3-point (95% confidence interval [CI] 0.2–2.4) verbal memory improvement across all participants.
Linear regression models examining the effect of left hippocampal volume and hippocampal asymmetry on the benefits of EPO on verbal learning
Does hippocampal volume asymmetry influence EPO treatment response for verbal memory?
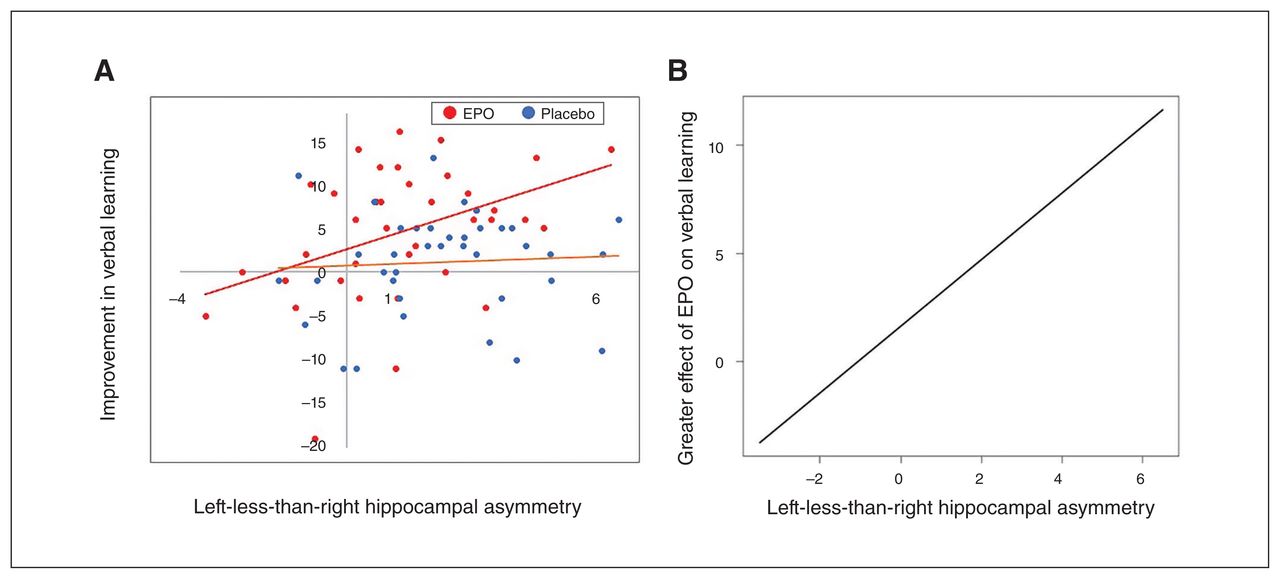
Rightward hippocampal asymmetry predicted enhanced treatment effects of EPO on verbal memory (p = 0.050; ηp2 = 0.06; Fig. 1). Specifically, we found a 54% greater improvement on the RAVLT total learning score following EPO treatment compared to placebo for every percent increase in HAI (95% CI 0.3–307; Table 2). Further, after adding baseline HDRS-17 scores, number of concomitant medications and whether patients received lithium as covariates, we found a similar significant association (p = 0.03).
{kind=link}
Association between (A) rightward hippocampal asymmetry and improvement in verbal learning from baseline to post-treatment across the 2 treatment groups, and (B) hippocampal asymmetry and greater effect of erythropoietin (EPO) on verbal memory.
Exploratory surface-based analysis
Do subregional PFC measurements influence EPO treatment response on verbal memory?
Within the PFC region of interest, we found a significant interaction effect between treatment group and baseline-to-follow-up changes in verbal memory scores in the left precentral gyrus surface area (adjusted p < 0.020). In this region, the linear regression slopes of changes in verbal memory were significantly different for the EPO and placebo groups (Appendix 1, Figure S1, available at jpn.ca/180205-a1). Specifically, a larger precentral surface area was associated with greater improvement in verbal memory in EPO-treated compared to placebo-treated participants. Analogue analyses using the cortical thickness and volume estimates did not show any significant findings. Across both treatment groups, we found no significant correlation in the PFC between changes in verbal memory and any of the 3 cortical representations. Rerunning the analyses with the search volume extended to the entire cortex revealed no additional regions with significant effects on EPO-related memory improvement.
Discussion
To our knowledge, this report demonstrates for the first time that interhemisphere hippocampal asymmetry influenced the efficacy of a treatment targeting cognition in patients with mood disorders. Specifically, reanalysis of the data from 76 patients in our EPO trials showed that greater rightward hippocampal asymmetry — but not left hippocampal volume — was associated with stronger treatment effects of EPO on verbal learning compared to placebo, with a medium effect size. Further, exploratory analysis suggested that a larger left precentral surface area, but not regional volume or thickness, influenced memory improvement in EPO-treated compared to placebo-treated patients.
The finding that patients with more rightward hippocampal asymmetry and larger left precentral gyrus surface area displayed greater EPO-related verbal memory improvement was consistent with the evidence that better brain reserve pretreatment is a predictor of treatment response for mood symptoms.10 This finding was also in keeping with the observation that people with schizophrenia who had a larger pretreatment cortical surface area and grey matter volume displayed more rapid social–cognitive improvement in response to cognitive enhancement therapy.45 Our findings thus contribute to the growing evidence that pretreatment brain reserve increases patients’ chances of treatment efficacy related to both mood and cognitive symptoms.10 The effect of greater rightward hippocampal asymmetry at baseline on the cognitive benefits of EPO may seem contradictory given our previous observation that EPO-related improvement of verbal learning was accompanied by increased subregional volume in the left hippocampus.46 However, this effect of EPO was merely within a subregion of the left hippocampus and had no effect on overall hippocampal asymmetry.
From a mechanistic perspective, this association between greater pretreatment brain reserve and better treatment efficacy may be explained by the fact that treatments capitalize on a surplus of neural capacity, which has the potential to induce more prominent functional reorganization and restitution of brain function. This could also explain why we found no support for the hypothesized association between smaller left hippocampal volume and EPO efficacy on verbal memory — a hypothesis that was based on our finding that pretreatment verbal memory impairment predicted greater cognitive benefits of EPO and on the suggestion by Wüstenberg and colleagues47 that EPO improves cognition by restoring lost neuroplasticity, such that those with more neuroplasticity loss would show the greatest treatment benefits. Instead, the present findings suggest that treatment efficacy in mood disorders is predicted by a greater rather than a poorer pretreatment brain reserve.
In contrast with the putative benefits of greater brain reserve for treatment efficacy with respect to both mood and cognition, pretreatment cognitive capacity seems to have the opposite effects for treatment efficacy in these symptom categories. Better cognition is a predictor of efficacy for mood symptoms, but poorer cognition seems to predict stronger treatment effects for cognitive impairment.10 Specifically, we had observed in the EPO trials that baseline memory deficits were associated with greater chances of EPO efficacy related to verbal memory,13 and that impairment on 2 or more of 6 cognitive tests predicted EPO efficacy for global cognition.14 This contrasting influence of brain reserve and cognitive capacity can seem counterintuitive. A possible explanation is that a combination of good brain reserve and poor cognition in EPO responders reflects less illness-related deterioration of brain functioning in the early course of illness, which occurs before structural brain changes and may be reversed by interventions targeting neuroplasticity. This would be in line with the “staging hypothesis” of neuropsychiatric illnesses, according to which cellular resilience mechanisms are more efficient at early illness stages, when patients also respond better to interventions,48 including lithium treatment49 and cognitive behavioural therapy.50 However, in post-hoc exploratory analyses we found no correlation between hippocampal asymmetry and the number of illness episodes or illness duration (number of episodes: β = −0.02, p = 0.42, 95% CI −0.07 to 0.3; illness duration: β = 0.01, p = 0.72, 95% CI −0.04 to 0.5) and no impact of illness chronicity on EPO-related verbal memory improvement (number of episodes: β = −0.05, p = 0.58, 95% CI −0.24 to 0.13; illness duration: β = 0.03, p = 0.69, 95% CI −0.12 to 0.17). Greater rightward hippocampal asymmetry may therefore not scale directly to lesser illness chronicity, but rather may reflect a larger premorbid brain reserve.
Limitations
A study limitation was the modest sample size (n = 76), which did not allow for more complex analyses of additional potential predictors; this would have resulted in suboptimal statistical power. Therefore, the findings should be considered only hypothesis generating. Further, because this report was a secondary analysis of our original EPO trials, our certainty is limited by the absence of replication in a new prospectively planned study. Nevertheless, a strength was that the analyses were based on some of the few randomized, controlled trials showing treatment-related cognitive improvement. The EPO patient cohort was thus uniquely suited for an investigation of baseline predictors of treatment efficacy on verbal memory.
Conclusion
Rightward hippocampal volume asymmetry may convey greater benefits of EPO treatment for verbal learning in patients with mood disorders. Future studies are warranted to investigate whether these findings are generalizable to other treatments — such as cognitive remediation in mood disorders — and to other neuropsychiatric illnesses. If so, rightward hippocampal volume asymmetry may be a predictor of treatment efficacy that can guide personalized treatments targeting cognition.
Footnotes
Funding: The Danish Council of Independent Research, Novo Nordisk Foundation, Beckett Fonden, and Savværksejer Juhl’s Mindefond are acknowledged for their financial support for the study. The sponsors had no role in the planning or conduct of the study or in the interpretation of the results. The Lundbeck Foundation and the Weimann Foundation are acknowledged for their contribution to K. Miskowiak’s salary from 2012 to 2020.
Competing interests: K. Miskowiak reports consultancy fees from Lundbeck, Allergan and Janssen within the past 3 years. M. Vinberg reports consultancy fees from Lundbeck within the last 3 years. H. Siebner has received honoraria as a speaker from Sanofi Genzyme and Novartis, as a consultant from Sanofi Genzyme and as senior editor of NeuroImage from Elsevier. He has received royalties as a book editor from Springer Publishers. He also holds a 5-year professorship in precision medicine at the Faculty of Health Sciences and Medicine, University of Copenhagen, that is sponsored by the Lundbeck Foundation (grant R186-2015-2138). L. Kessing reports having been a consultant for Lundbeck, AstraZeneca and Sunovion within the last 3 years. No other authors report competing interests.
Contributors: K. Miskowiak, M. Vinberg, H. Siebner, L. Kessing, and J. Macoveanu designed the study. K. Miskowiak acquired the data, which K. Miskowiak, J. Forman and J. Macoveanu analyzed. K. Miskowiak and J. Macoveanu wrote the article, which all authors reviewed. All authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
- Received October 29, 2018.
- Revision received May 29, 2019.
- Accepted July 26, 2019.