Article Text

Abstract
Background Polymorphisms of the gene encoding the serotonin transporter—specifically, length variation in the serotonin-transporter-linked polymorphic region (5-HTTLPR), a single-nucleotide polymorphism in the 5-HTTLPR (rs25531), and variable number of tandem repeats (VNTR) in the second intron 2 (STin2)—have been implicated in the development of post-stroke depression (PSD).
Objective To evaluate the association between polymorphisms of the serotonin transporter gene and PSD in the medical literature.
Methods Random-effects meta-analyses were conducted on cross-sectional, case–control and cohort studies examining relations between polymorphisms of the gene encoding the serotonin transporter and the risk of developing PSD.
Results Four studies comprising 260 stroke patients with PSD and 381 without were included. Our analyses showed a significant and positive association between the homozygous short variation (S) allele genotype of the 5-HTTLPR (SS) and PSD (random-effects pooled OR 2.05, 95% CI 1.41 to 2.98, z=3.79, p<0.001). Our analyses also showed a significant and negative association between the homozygous long variation (L) allele genotype of the 5-HTTLPR (LL) and PSD (random-effects OR 0.52, 95% CI 0.27 to 0.97, z=−2.07, p=0.039). No statistically significant association of PSD with heterozygous S and L allele genotype for 5-HTTLPR or other polymorphisms with rs25531 and STin2 VNTR was found. Heterogeneity and publication bias were not statistically significant. The major limitation of this meta-analysis is that we could not assess the interaction between stroke, environmental stress and PSD.
Conclusions The 5-HTTLPR SS genotype may be a risk factor for PSD. The 5-HTTLPR LL genotype showed a significant negative association with PSD. Further research to assess the sensitivity and specificity of predicting the risk of developing PSD by screening for the 5-HTTLPR genotype in stroke patients is required.
- Meta-Analysis
- Stroke
- Depression
- Genetics
Statistics from Altmetric.com
Introduction
Post-stroke depression (PSD) is a common psychiatric phenomenon that affects nearly 30% of stroke patients at some stage.1 Impaired functioning of the serotoninergic system is involved in the pathogenesis of depressive disorders and regulated by the serotonin transporter gene. The gene that encodes the serotonin transporter, known as solute carrier family 6, member 4 (SLC6A4), can be found on chromosome 17 at the location 17q11.1-q12.2 Variations associated with the serotonin transporter gene include length variation in the serotonin transporter gene-linked polymorphic region (5-HTTLPR), a single-nucleotide polymorphism in the 5-HTTLPR (rs25531), and a variable number of tandem repeats (VNTR) in the second intron 2 (STin2).3
Length variation in the 5-HTTLPR is typically defined by two variable nucleotide tandem repeat elements. The short variation (S) allele of the 5-HTTLPR polymorphism leads to 14 repeats of base pair sequences. In contrast, a long variation (L) allele leads to 16 repeats of base pair sequences. The S allele of the 5-HTTLPR polymorphism leads to a reduction in transcription efficiency for SLC6A4, basal serotonin activity, serotonin binding, amount of grey matter in the anterior cingulate gyrus and amygdale,4 as well as anxiety personality traits.5 Whereas most studies found no significant associations between PSD and homozygous LL alleles of the 5-HTTLPR,6–8 one study showed a significant inverse association, with an OR of 0.15.9 Regarding relations between PSD and the homozygous SS alleles of the 5-HTTLPR, contradictory results have been reported. rs25531, a single-nucleotide polymorphism closest to the 5-HTTLPR that results in an A–G substitution, modulates the effect of the 5-HTTLPR on transcription efficacy. Although the G allele of rs25531 is in phase with the 5-HTTLPR L allele,10 neither rs25531 AA nor rs25531 AG/GA have been found to be associated with PSD.6 ,9 ,11 Finally, VNTR in the STin2 has three alleles (9, 10 and 12 repeats). The 9 and 10 repeats are considered to be S alleles, and the 12 repeats are considered to be L alleles.12 The S and L alleles are purported to increase transcription of the serotonin transporter gene.13 Although STin2 VNTR polymorphism is not associated with mood disorders, its association with PSD remains controversial.14
The objective of this meta-analysis was to evaluate the association between variations in the serotonin transporter gene and PSD. We performed a meta-analysis of cross-sectional, case–control and cohort studies to determine the overall strength of the putative association between PSD and polymorphisms of the 5-HTTLPR, rs25531 and STin2 VTNR in stroke patients.
Methods
The review process was based on the following protocol. Online databases (PubMed, Embase, PsychINFO, BIOSIS and Science Direct) were searched from inception to October 2011. The search items used were a combination of keywords for post stroke (‘post stroke, post cerebral infarction, post cerebral vascular accident, post cerebral ischaemia, post cerebral haemorrhage’), depression (‘depression, depressive disorder, minor depressive disorder and dysthymia’) and genotype (‘genotype, genetic, genetic association studies, genotyping techniques, serotonin transporter genes, 5-HTTLPR genes, STin2 VNTR genes and rs25531 genes’). The search was limited to articles that reported data from humans and published in the English language. Abstracts presented in major international conferences were manually searched, and the authors of correspondence were contacted for further information. References from retrieved papers were also considered. We sought all cross-sectional, case–control and cohort studies that examined the relationship between PSD and serotonin transporter genotype variations. Studies were included if they: (1) were case–control studies or prospective studies; (2) analysed a blood/saliva sample for DNA and genotypes as the main variable of interest or as a covariate; (3) analysed PSD as the dependent variable where stroke was confirmed by imaging studies or medical records and depression was assessed clinically by structured psychiatric diagnostic interview; (4) provided sufficient information to calculate the effect size. For case–control studies to be included, studies must have drawn some comparison between the presence of a particular serotonin transporter genotype variation and the presence of PSD. Furthermore, they must have used stroke patients without PSD as a reference group for comparisons. For inclusion of prospective studies in the meta-analysis, sufficient information was required to estimate OR. Studies were excluded if the subjects studied had a medical record of previously diagnosed depression (including self-reported depression). In addition, we excluded case reports and case series. Selection of relevant publications was conducted independently by two authors (WYK and RCMH). Articles were initially screened on the basis of titles and abstracts. The short-listed articles were then evaluated for study design and screened for the inclusion and exclusion criteria listed above. Disagreement regarding inclusion or exclusion of the retrieved papers was resolved by discussion before the final set of articles used in this meta-analysis was produced.
Statistical methods
Data extraction
The following information was extracted from each article, cross-checked by the second researcher, and recorded on a standardised data collection form: (a) demographics of participants—for example, mean age, proportion of gender, proportion of ethnicities; (b) duration of stroke; (c) genotype of the 5HTLPR; (d) outcomes, description of instruments assessing PSD, the number of PSD cases versus controls for each 5-HTTLPR genotype.
Statistical analysis
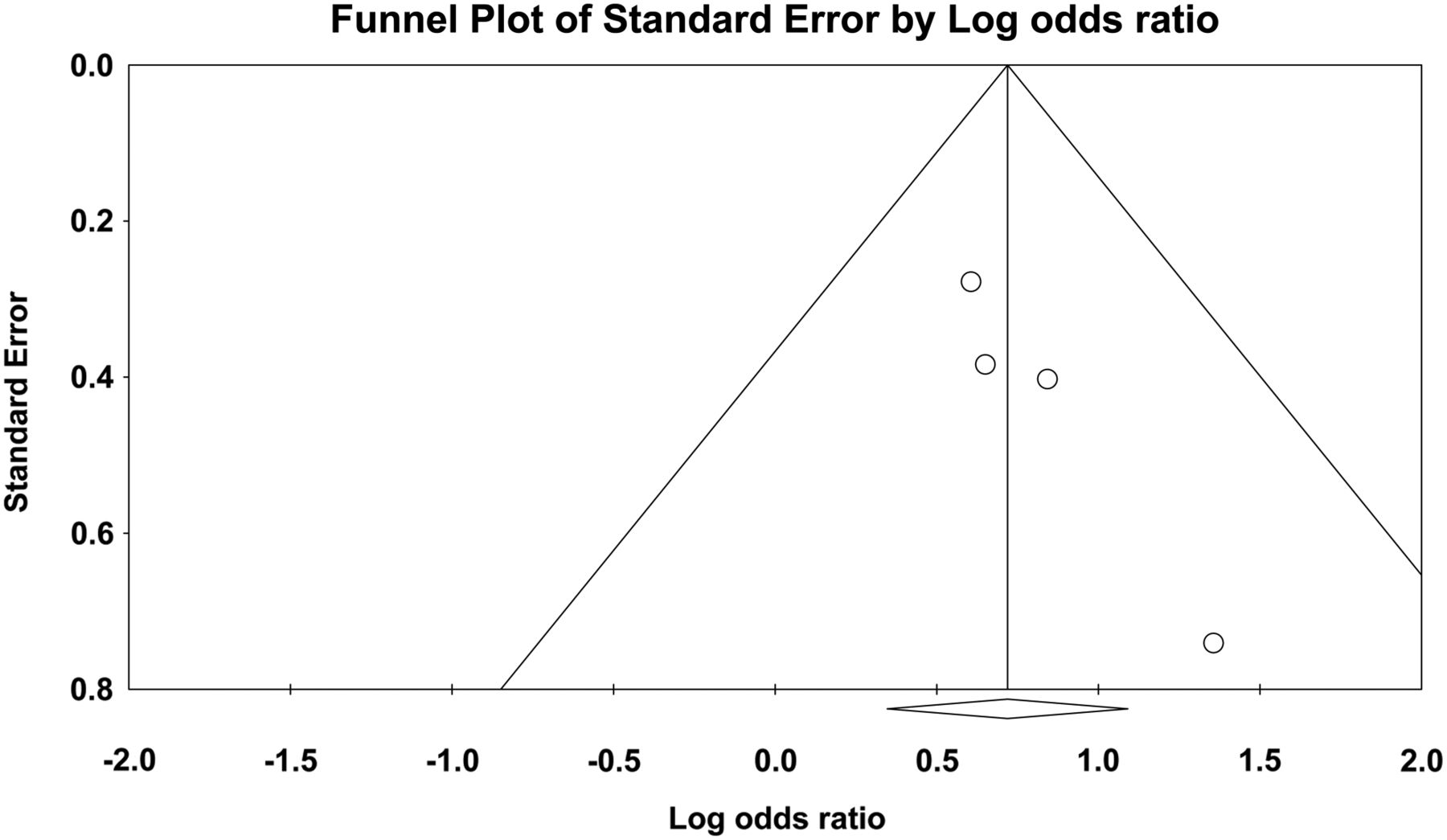
All statistical analyses were performed with Comprehensive Meta-Analysis V.2.0 using random-effects models. All trials reported PSD and no depression after stroke as dichotomous outcomes. Thus, summary statistics including OR and 95% CIs were calculated for each study. To test the hypothesis that a specific polymorphism is in fact the risk allele for PSD, the pooled OR was calculated using a random-effects model. The random-effects model was used because it is more conservative by providing a narrower CI than the fixed-effects model. The pooled OR, 95% CI, z and p values were reported for each 5-HTTLPR genotype. Significant difference was set at p<0.05 for all analyses. Between-study heterogeneity was assessed with the I2 statistic, which describes the percentage of variability among effect estimates beyond that expected by chance.15 As a reference, I2 values of 25% were considered low, 50% moderate, and 75% high. For results with considerable and significant heterogeneity, meta-regression would be performed to identify patient-related factors (mean age, proportion of gender, proportion of ethnicity and mean duration of stroke) that might contribute to the heterogeneity of effect sizes. Funnel plots and Egger regression tests for funnel plot asymmetry were performed to detect publication bias. If significant publication bias was present, a classic fail-safe test was performed to identify the number of missing studies that would bring the p value of publication bias among the observed studies to >0.05.
Results
Four studies with a total of 260 patients with PSD and 381 patients without PSD were included in the analysis (figure 1). The studies consisted of patients from Western as well as Asian countries. Baseline characteristics of the study populations are shown in table 1.
Descriptive characteristics of four case–control studies between the 5-HTTLPR polymorphism and post-stroke depression (PSD)

Literature search profile.
The 5-HTTLPR genotype
Figures 2 ⇓–4 show the results of four studies that compared the presence of 5-HTTLPR LL, SS and SL genotype, respectively, between patients with PSD and those without. The proportion of patients with the 5-HTTLPR LL genotype is significantly lower in the PSD group than in the group without PSD (pooled OR 0.52, 95% CI 0.27 to 0.97, z=−2.065, p=0.039). The between-study heterogeneity was small but not statistically significant (τ2=0.143, Q=4.6, df=3, p=0.2, I2=34.8). As a result, meta-regression was not performed. The proportion of patients with the 5-HTTLPR SS genotype is significantly higher in the PSD group than in the non-PSD group (pooled OR 2.05, 95% CI 1.41 to 2.98, z=3.79, p<0.001). No between-study heterogeneity was found (τ2=0, Q=1.03, df=3, p=0.79, I2=0). As a result, meta-regression was not performed. The proportion of participants with the 5-HTTLPR SL genotype appears to be lower in the PSD group than in the non-PSD group, but the result is not statistically significant (pooled OR 0.75, 95% CI 0.53 to 1.07, z=−1.58, p=0.12) . No between-study heterogeneity was found (τ2=0, Q=1.24, df=3, p=0.74, I2=0). As a result, meta-regression was not performed.

Homozygous serotonin transporter-linked polymorphic region long variation allele genotype meta-analysis. PSD, post-stroke depression.

Homozygous serotonin transporter-linked polymorphic region short variation allele genotype meta-analysis. PSD, post-stroke depression.

Heterozygous serotonin transporter-linked polymorphic region (SL) genotype meta-analysis. PSD, post-stroke depression.
The rs25531 genotype
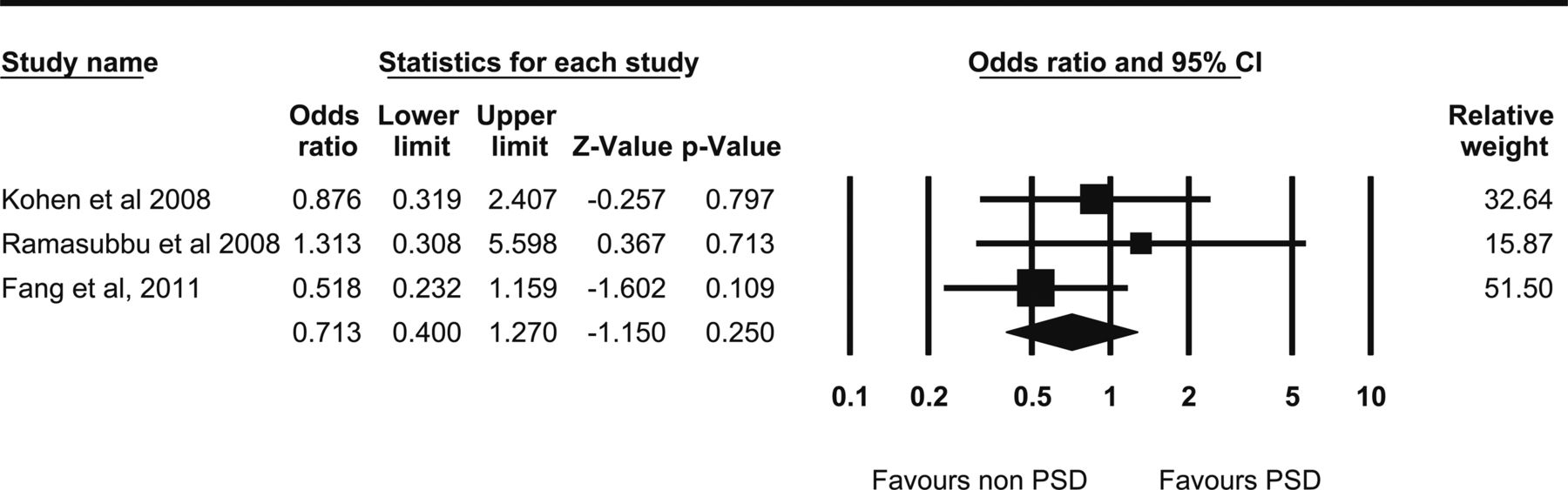
Figures 5 and 6 show the results of three studies that compared the presence of rs25531 AA genotype and rs25531 AG genotype, respectively, between patients with PSD and those without. The proportion of participants with the rs25531 AA genotype appears to be lower in the PSD group than in the non-PSD group, but the result is not statistically significant (pooled OR 0.71, 95% CI 0.40 to 1.27, z=−1.15, p=0.25). No between-study heterogeneity was found (τ2=0, Q=1.44, df=2, p=0.49, I2=0). As a result, meta-regression was not performed. The proportion of patients with the rs25531 AG/GA genotype seems to be higher in the PSD group than in the non-PSD group, but again the result is not statistically significant (pooled OR 1.28, 95% CI 0.63 to 2.59, z=0.69, p=0.49). No between-study heterogeneity was found (τ2=0, Q=0.47, df=2, p=0.79, I2=0). As a result, meta-regression was not performed.
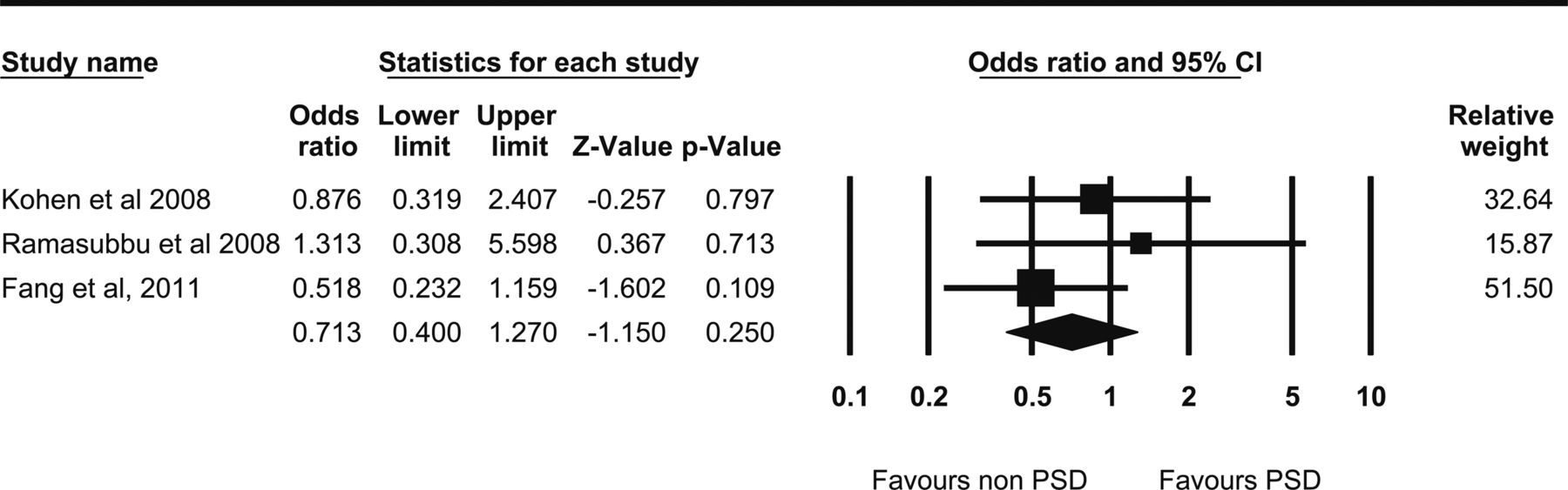
rs25531 AA genotype meta-analysis. PSD, post-stroke depression.

rs25531 AG genotype meta-analysis. PSD, post-stroke depression.
The STin2 VNTR genotype
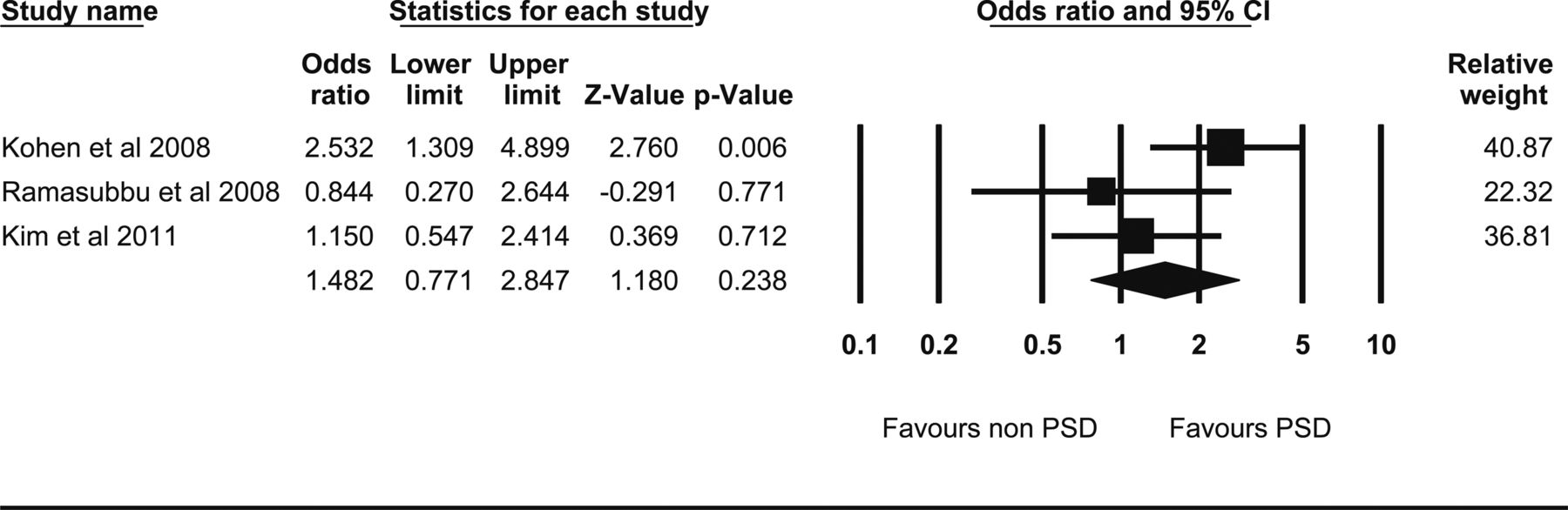
Figures 7 and 8 show the results of three studies that compared the presence of STin2 VNTR 10/12 and 12/12 or 9/12 genotype, respectively, between patients with PSD and those without. The proportion of participants with the STin2 VNTR 10/12 genotype is lower in the PSD group than in the non-PSD group, but the result is not statistically significant (pooled: 0.71, 95% CI 0.45 to 1.12, z=−1.47, p=0.14). No between-study-heterogeneity was found (τ2=0, Q=1.98, df=2, p=0.37, I 2=0). As a result, meta-regression was not performed. The proportion of participants with the STin2 VNTR 12/12 or 9/12 genotype seems to be higher in the PSD group than in the non-PSD group, but the result is not statistically significant (pooled OR with random effects model: 1.48, 95% CI 0.77 to 2.84, z=1.18, p=0.24). The between-study heterogeneity was small, but not statistically significant (τ2=0.16, Q=3.83, df=2, p=0.15, I2=47.73). As a result, meta-regression was not performed. There were only two studies that compared the presence of the STin2 VNTR 10/10 genotype between patients with PSD and those without. The number of participants with the STin2 VNTR 10/10 genotype is lower in the PSD group than in the non-PSD group, but the result is not statistically significant (pooled OR 0.65, 95% CI 0.28 to 1.49, z=−1.02, p=0.31). There was no between-study heterogeneity (τ2=0, Q=0.44, df=1, p=0.51, I2=0) and there were only two studies. As a result, meta-regression was not performed.

Second intron 2 variable number of tandem repeats 10/12 genotype meta-analysis. PSD, post-stroke depression.

Second intron 2 variable number of tandem repeats 12/12 or 9/12 genotype meta-analysis. PSD, post-stroke depression.
Publication bias
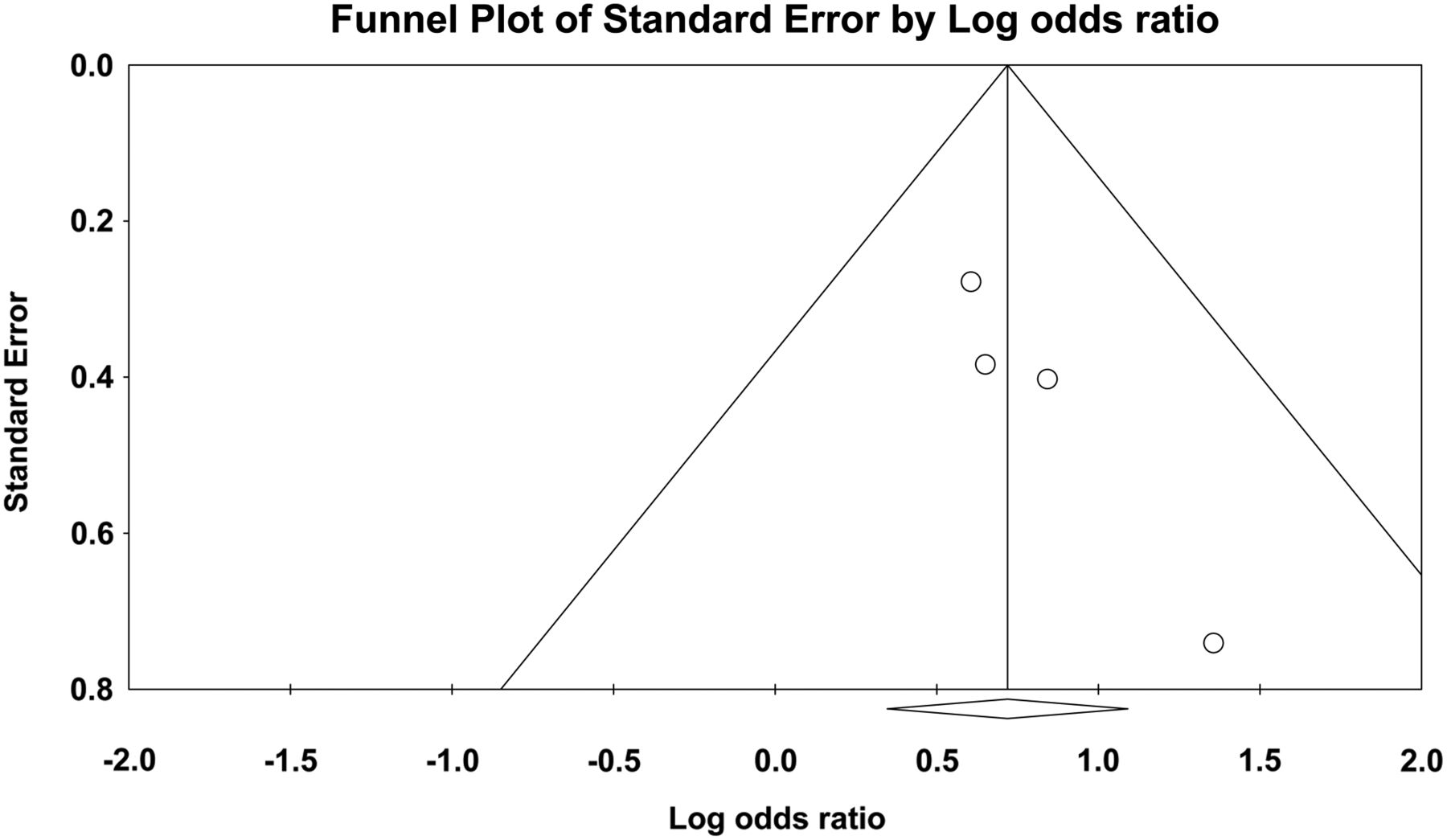
There was no significant publication bias for any of the gene polymorphisms: 5-HTTLPR LL (p=0.09), 5-HTTLPR LS (p=0.458), rs25531 AA (p=0.194), rs25531 AG (p=0.956), STin2 VNTR 10/12 (p=0.354) and STin2 VNTR 12/12 (p=0.47). The statistical significance level of publication bias for the 5-HTTLPR SS genotype between the PSD and non-PSD group was marginal (intercept=1.59, 95% CI −0.01 to 3.20, τ=4.27, df=2, p=0.051) (figure 9). On the basis of the classic fail safe test, 12 missing studies are required for every observed study to nullify the effect.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot for the 5-serotonin transporter-linked polymorphic region short variation allele genotype meta-analysis.
Discussion
To our knowledge, this is the first meta-analysis investigating the 5-HTTLPR, rs25531 and STin2 VNTR polymorphisms and PSD. The opposite findings for the relationship between 5-HTTLPR SS and LL alleles and PSD may suggest their different roles in emotion regulation and the risk of developing depression in stroke patients. Previous studies have demonstrated that S alleles increase vulnerability to development of major depressive disorders in women who experience stressful life events.16 ,17 The S allele of the 5-HTTLPR results in lower expression of the SLC6A4 gene. This gene encodes an integral membrane protein that transports the neurotransmitter, serotonin, from synapses to presynaptic neurons.3 A repeat-length polymorphism in the promoter of this gene has been shown to affect the rate of serotonin uptake and has been reported to be associated with anxiety-related personality traits, suicidal behaviour and depression.5 ,14 ,16 ,18 The association between the S allele of the 5-HTTLPR and the lower expression of SLC6A4 not only affects the action of serotonin but also causes cytoarchitectonic changes and density reduction in the somatosensory cortex in rats.19 ,20 Pezawas et al 4 reported that S allele 5-HTTLPR carriers have significantly reduced amygdale–anterior cingulated cortex connectivity compared with homozygous LL allele 5-HTTLPR carriers. Somatosensory deficit syndrome is a common impairment following stroke and has a prevalence of ∼80% in post-stroke patients.21 Interestingly, these disturbances are common features of PSD.
Our results may suggest a role for the serotonin transporter gene in risk of stroke, as this gene plays a critical part in regulating food intake, body weight and energy balance.22 Way and Taylor reported that homozygosity for 5-HTTLPR S alleles is associated with high cardiovascular reactivity to stress in a threatening environment.23 Indeed, previous studies have demonstrated that the 5-HTTLPR SS genotype is associated with adverse cardiac outcomes, including an increase in carotid artery intima–media thickness24 and hypertension.25 Homozygosity for the SLC6A4 S allele has been reported to be associated with higher diastolic blood pressure, systolic blood pressure, mean arterial blood pressure and plasma triglyceride.26 The adverse cardiac and metabolic outcomes27 are the result of a reduction in serotoninergic neurotransmission.28–30 Hoffman et al 31 found that adult female rhesus monkeys with the S allele in the 5-HTTLPR had metabolic alterations and suggested the possibility that the SS genotype may predispose them to further metabolic deficits when exposed to psychosocial stressors. Lan et al 32 also reported that the 5-HTTLPR SS genotype is an independent determinant of obesity in non-elderly stroke patients. Kim et al 33 conducted a prospective study of older Koreans and found associations between lower baseline levels of high-density lipoprotein, prevalent and incident depression, and the presence of one or more copies of the S allele of the 5-HTTLPR genotype. Future research is required to explore the relationship between polymorphisms of the 5-HTTLPR genotype, cardiovascular risk and PSD.
The present meta-analysis also serves as a preliminary overview of the role of genetics as a potential aetiological factor in PSD. Further longitudinal studies are required to study the interaction between length variation alleles in the 5-HTTLPR and stroke in the causation of PSD. Such studies should provide information on the sensitivity and specificity of predicting the risk of PSD development by screening for the 5-HTTLPR genotype in stroke patients. Early treatment and prophylaxis with antidepressants against PSD in stroke patients with the homozygous 5-HTTLPR SS genotype may be a future therapeutic possibility. Although early antidepressant treatment may offer benefits such as reduction in depression scores and suicidal rate and improvement in quality of life, antidepressants may lead to risks such as hyponatraemia and bleeding tendency. Therefore, further information is required from risk–benefit analysis before early antidepressant treatment for PSD can be recommended.
In this meta-analysis, the polymorphisms rs25531 and STin2 VTNR did not show any association with PSD. This negative finding is similar to earlier findings of no association between suicide attempt or ideation and the rs25531 and STin2 VTNR haplotype distribution.10 However, polymorphisms of rs25531 and STin2 VTNR influence transcription efficacy of the serotonin transporter gene. In this meta-analysis, the pooled ORs for heterozygous A and G alleles for rs25531, heterozygous 9 and 12 repeats and homozygous 12 and 12 repeats of STin2 VNTR were 1.28 and 1.51, respectively. These statistically insignificant findings warrant further studies with a larger sample size.
This meta-analysis has a number of limitations. First, the association between the homozygous 5-HTTLPR SS genotype and PSD should be interpreted cautiously because there are other factors that may confound such an association—for example, gender, ethnicity and season of birth. The interaction between polymorphisms of 5-HTTLPR and stress is influenced by gender. Brummett et al 34 found that the homozygous 5-HTTLPR SS genotype is associated with an increase in susceptibility to depression during stressful life events in women. In contrast, the homozygous 5-HTTLPR LL genotype is associated with depression during stressful life events in men. In our meta-analysis, the odds of developing PSD were not related to gender. We performed further analysis and found that 55.3% of patients with PSD and 61.4% of patients without were men. The odds of male gender in the PSD group are no higher than in the control group (pooled OR 0.748, 95% CI 0.51 to 1.097, z=−1.487 and p=0.137). It is reasonable to postulate that the relationship between serotonin transporter genes and PSD may be modified by ethnicity, similarly to previous meta-analyses of polymorphisms in serotonin transporter genes in patients with migraine35 and autism.36 Further study is required on ethnic groups other than Caucasians and East Asians—the only ethnic groups studied in this meta-analysis. The season of birth may affect the frequency of the 5-HTTLPR S allele in depressed patients. Chotai et al 37 reported that depressed men and women with homozygous 5-HTTLPR SS alleles were more likely to have been born between October and March and between May and July, respectively. The season of birth was not analysed in the primary studies. As a result, we were not able to study the relationships among season of birth, serotonin transporter gene polymorphism and PSD in this meta-analysis.
Wankerl et al 38 highlighted the major limitation of meta-analysis for studying the relationship between the 5-HTTLPR polymorphisms and depression. Meta-analysis usually combines similar studies with rigid selection criteria. This is known to be an exclusive approach because it is methodologically inappropriate to combine studies with different methods and designs, which are important to address the interaction between genotype and environment.38 This limitation also applies to our study. We could not assess the interaction between stroke, environmental stress and PSD because not all studies included assessed environmental stress. This limitation is further complicated by the absence of a consistent approach to measuring environmental stress in depression research focusing on the gene–environment interaction.39
One further weakness of the present meta-analysis is the presence of publication bias with marginal statistical significance (p=0.05) in the finding of the association between the 5-HTTLPR SS genotype and PSD. The cause of this potential publication bias is the small number of studies included, and these studies were published in English. In this mete-analysis, we focused on serotonin gene polymorphisms because there is a paucity of studies exploring the relationship between PSD and other polymorphisms linked to depression. Further research is required to study the relationship between PSD and polymorphisms of the dopamine receptor D2 (DRD2) gene and the brain-derived neutrophic factor gene.
In conclusion, the present meta-analysis found a significant positive association between the 5-HTTLPR SS genotype and PSD and a significant negative association between the 5-HTTLPR LL genotype and PSD. No significant association was found between heterozygous S and L allele genotypes for 5-HTTLPR, single-nucleotide polymorphisms of rs25531 and STin2 VTNR and PSD. Thus, 5-HTTLPR may be a serotonin system candidate gene for PSD. To further understand the relationship between allele length variation of the serotonin transporter gene and stroke in causing PSD, more prospective studies with larger sample sizes and different ethnicities are required.
References
Footnotes
-
Contributors K-KM: contributed to development of the research idea and design, drafted the introduction and discussion, and gave approval for the final version to be published. WYK: contributed to development of the research idea and acquisition of data, or analysis and interpretation of data, drafted the methodology and results sections and prepared the forest plots, tables and figures, and gave approval for the final version to be published. AM: contributed to development of the research idea and interpreted the data, revised the manuscript and provided expert and critical comments on the meta-analysis, and gave approval for the final version to be published. VKS: contributed to development of the research idea and interpreted the data, revised the manuscript, references and provided expert advice from a neurology perspective, and gave approval for the final version to be published. RCMH: contributed to design, acquisition of data, or analysis and interpretation of data, wrote the introduction and discussion and revised the whole paper critically, gave approval for the final version to be published, finalised replies to reviewers, and is guarantor of the work.
-
Funding None.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentaries
- Editorial commentary