
Abstract
Objective
The aim of this study was to determine the extent and patterns of antidepressant use before, during and after pregnancy in a large population in The Netherlands.
Methods
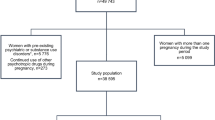
Health care records and prescription data from one of the largest Dutch health insurance companies were analysed. The study cohort consisted of 29,005 women who had live births in the period between January 2000 and July 2003. Antidepressant drug use during a specified period was defined as there being a record of a prescription during that period.
Results
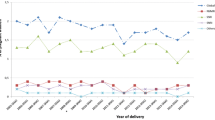
During the first trimester of pregnancy 2% of all pregnant women of the study cohort were found to have taken antidepressants; in the second and third trimesters, this figure had dropped to 1.8% of all pregnancies. Antidepressant use before as well as during pregnancy was almost twofold higher in women over 35 years of age than in those under 35 years. Almost 60% of the women who used antidepressants before pregnancy stopped taking them in the first trimester, and a smaller number stopped thereafter. Of all women using antidepressants during pregnancy, one third started this medication during gestation. In the 3 months following delivery, the prevalence of antidepressant use was the same as before pregnancy (2.9%). There was no shift to benzodiazepines in the group of women who stopped taking antidepressants during pregnancy. Although paroxetine and fluoxetine were the most frequently used antidepressants among the study group, all modern antidepressants were used.
Conclusion
A considerable number of women are being exposed to antidepressants throughout pregnancy up until delivery. One consequence of this is that their newborns need special care and supervision during the first days of life. However, women who stop taking the medication may risk a relapse of their illness, and this may also have a negative effect on the child.
Similar content being viewed by others

References
Hansen DG, Sondergaard J, Vach W, Gram LF, Rosholm JU, Kragst J (2003) Antidepressant drug use in general practice: inter-practice variation and association with practice characteristics. Eur J Clin Pharmacol 59:143–149
De las Cuevas C, Sanz E (2004) Do therapeutic indications of antidepressants change from one year to another? Pharmacoepidemiol Dr S 13:309–314
Foundation for Pharmaceutical Statistics, Farmacie in cijfers. [Pharmacy in figures. Drug use of antidepressants is increasing] 2005 Pharmaceutisch Weekblad 140:767 or http://www.sfk.nl/publicaties/farmacie_in_cijfers/2005
Kallen B, Otterblad Olausson P (2006) Antidepressant drugs during pregnancy and infant congenital heart defect. Reprod Toxicol 21:221–222
Williams M, Wooltorton E (2005) Paroxetine(Paxil) and congenital malformations. Can Med Assoc J 173:1320–1321
Casper RC, Fleisher BE, Lee-Ancajas JC, Gilles A, Gaylor E, DeBattista A, Hoyme HE (2003) Follow-up of children of depressed mothers exposed or not exposed to antidepressant drugs during pregnancy. J Pediatr 142:402–408
Zeskind PS, Stephens LE (2004) Maternal Selective serotonin reuptake inhibitor use during pregnancy and newborn neurobehavior. Pediatrics 113:368–375
Chambers CD, Hernandez-Diaz S, Van Marter LJ, Werler MM, Louik C, Jones KL, Mitchell AA (2006) Selective serotonin-reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. N Engl J Med 354:579–587
Nonacs R, Cohen LS (2003) Assessment and treatment of depression during pregnancy: an update. Psychiatr Clin N Am 26:547–562
Sanz EJ, De-las-Cuevas D, Kiuru A, Bate A, Edwards R (2005) Selective serotonin reuptake inhibitors in pregnant women and neonatal withdrawal syndrome: a database analysis. Lancet 365:482–487
Olesen C, Sorensen HT, de Jong-van den Berg L, Olsen J, Steffensen FH (1999) Prescribing during pregnancy and lactation with reference to the Swedish classification system. A population-based study among Danish women. The Euromap Group. Acta Obstet Gynecol Scand 78:686–692
Beyens MN, Guy C, Ratrema M, Ollagnier M (2003) Prescription of drugs to pregnant women in France: the HIMAGE study. Therapie 58:505–511
Schirm E, Meijer WM, Tobi H, de Jong-van den Berg LT (2004) Drug use by pregnant women and comparable non-pregnant women in the Netherlands with reference to the Australian classification system. Eur J Obstet Gynecol Reprod Biol 114:182–188
Headley J, Northstone K, Simmons H, Golding J; ALSPAC Study Team (2004) Medication use during pregnancy: data from the Avon longitudinal study of parents and children. Eur J Clin Pharmacol 60:355–361
Egen-Lappe V, Hasford J (2004) Drug prescription in pregnancy: analysis of a large statutory sickness fund population. Eur Clin Pharmacol 60:659–666
Andrade SE, Gurwitz JH, Davis RL, Chan KA, Finkelstein JA, Fortman K, McPhillips H, Raebel MA, Roblin D, Smith DH, Yood MU, Morse AN, Platt R (2004) Prescription drug use in pregnancy. Am J Obstet Gynecol 191:398–407
Czeizel AE, Petik D, Vargha P (2003) Validation studies of drug exposures in pregnant women. Pharmacoepidemiol Dr S 12:409–416
Schirm E, Tobi H, de Jong-van den Berg LTW (2004) Identifying parents in pharmacy data: a tool for the continuous monitoring of drug exposure to unborn children. J Clin Epidemiol 57:737–741
Mittendorf R, Williams MA, Berkey CS, Cotter PF (1990) The length of uncomplicated human gestation. Obstet Gynecol 75:929–932
Australian Drug Evaluation Committee. Medicines in Pregnancy Working Party, Prescribing Medicines in Pregnancy. Australian categorisation of drugs, 4th ed. [cited 3 September 2004]. Available from URL: http://www.health.gov.au/tga/docs/html/medpreg.htm
Statistics Netherlands (CBS) Voorburg, the Netherlands. Available from URL: http://www.cbs.nl/enGB/default.htm
Nulman I, Rovet J, Stewart DE, Wolpin J, Pace-Asciak P, Shuhaiber S, Koren G (2002) Child development following exposure to tricyclic antidepressants or fluoxetine throughout fetal life: a prospective, controlled study. Am J Psychiatry 159:1889–1895
Nordeng H, Spigset O (2005) Treatment with selective serotonin reuptake inhibitors in the third trimester of pregnancy. Drug Safety 28:565–581
Cohen LS, Altshuler LL, Stowe ZN, Faraone SV (2004) Reintroduction of antidepressant therapy across pregnancy in women who previously discontinued treatment. A preliminary retrospective study. Psychother Psychosom 73:255–258
Jaiswal S, Coombs RC, Isbister GK (2003) Paroxetine withdrawal in a neonate with historical and aboratory confirmation. Eur J Pediatr 162:723–724
Gentile S (2005) SSRIs in pregnancy and lactation: emphasis on neurodevelopmental outcome. CNS Drugs 19:623–633
Hines RN, Adams J, Buck GM, Faber W, Holson JF, Jacobson SW, Keszler M, McMartin K, Segraves RT, Singer LT, Sipes IG, Williams PL (2004) NTP-CERHR Expert Panel Report on the Reproductive and Developmental Toxicity of Fluoxetine. Birth Defects Res Part B71:193–280
Kallen B (2004) Fluoxetine use in early pregnancy. Birth Defects Res Part B 71:395–396
Acknowledgement
We are grateful to the VGZ Health Insurance Company for providing the health care and medication records we used in our study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Mr. H. Kaasenbrood died on October 14, 2005.
Rights and permissions
About this article
Cite this article
Ververs, T., Kaasenbrood, H., Visser, G. et al. Prevalence and patterns of antidepressant drug use during pregnancy. Eur J Clin Pharmacol 62, 863–870 (2006). https://doi.org/10.1007/s00228-006-0177-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-006-0177-0