
Abstract
Objective: It is very challenging to make an unbiased diagnosis of psychiatric illness. Platelets have long been proposed as easily obtainable, neurological models of serotonergic neurons. This study examined whether a new measurement for platelet serotonin could aid in the diagnosis of postpartum depression and support the results from questionnaires.
Methods: Study participants included 11 patients with postpartum clinical depression according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, criteria. Blood was donated either at acute onset of depression before treatment (n = 5) or while patients were nonresponsive to paroxetine treatment (n = 8; 2 of these patients dropped out). A follow-up sample was donated approximately 8 weeks later during paroxetine treatment (n = 11). Platelet serotonin was determined with a new immunocytochemical assay and standard high-pressure liquid chromatography. Serotonin levels were compared with Hamilton Depression Rating Scale scores.
Results: Platelet serotonin levels in patients with depression before paroxetine treatment or nonresponsive to their initial paroxetine regimen were reduced to 50% of normal levels. Treatment-induced severe reduction of platelet-associated serotonin only occurred in responsive patients. Mean platelet serotonin levels were significantly lower in responders (17.3%, standard deviation [SD] 4%), compared with nonresponders (33.4%, SD 8%; p < 0.001).
Conclusion: Platelet serotonin levels obtained with a new immunocytochemical test correlated well with results from depression scoring and might be useful as evidence-based support for questionnaires.
Introduction
The postpartum period is considered a time of increased risk for the onset and recurrence of mood and anxiety disorders1 and affects 10%–15% of women in western countries. Postnatal depression is increasingly recognized as a public health concern, since it is the leading cause for maternal morbidity and mortality and has adverse long-term effects on infants and families, in particular, in western countries.2 Thus it is of paramount importance to treat mothers with postpartum depression effectively.3–5
Major depressive disorder (MDD) postpartum onset, although similar in clinical presentation to nonpostpartum depression, is often accompanied with higher levels of comorbid anxiety.6 In terms of biological and genetic vulnerability underlying this illness, the exact mechanism has not been elucidated; however, there appears to be a strong familial connection with blood relatives who show a history of mood disorders.7
One problem in interpreting treatment effectiveness is the lack of confidence in psychometric tools. The diagnosis and rating of the severity of postpartum depression is currently based on subjective rating scales, such as the 21-item Hamilton Depression Rating Scale (HAM-D)8 and the Edinburgh Postnatal Depression Scale (EPDS).9
Over the last 3 decades, evidence has accumulated that supports a preeminent role for serotonergic dysfunction in the pathophysiology of depression.10–14 Consequently, selective serotonin reuptake inhibitors (SSRIs) have been found to be highly effective in the treatment of depression.15–17
For many years, a marker in peripheral blood was sought that could aid psychiatrists with the diagnosis of depression and the dosing of antidepressant drugs. Peripheral serotonin has long been proposed to be the ideal marker,18 because blood serotonin is contained in platelets. Platelets also share a similar serotonin uptake and release mechanism with serotonergic neurons.19–21 In addition, peripheral and brain serotonin might be linked, because the blood–brain barrier seems to act as a regulatory interface for neurotransmitters. Especially under stressful conditions, circulating serotonin is able to cross the blood–brain barrier in humans and experimental animals.22–24 The invention and use of SSRIs have stimulated research on platelet serotonin as a marker for depression and treatment efficacy since the 1970s. However, these studies investigated platelet uptake and release of externally added and usually radio-labelled serotonin as a marker of depression and response to treatment.25–32 Research focused on serotonin transport across the platelet membrane rather than the actual platelet serotonin content. Because these studies arrived at controversial results, it was concluded that platelet serotonin measurements are physiologically not relevant for depression.
We revisited this issue of platelet serotonin as a biomarker, using our new immunocytochemical method to determine platelet serotonin.33,34 This assay measures the platelet serotonin content at the time of blood donation. Because of its ease of use, platelet serotonin measurements could be performed routinely to support the results obtained with questionnaires. The absence of a circadian rhythm of platelet serotonin levels has been shown,35,36 although a circadian rhythm of platelet serotonin uptake and release exists.37 Maurer-Spurej and colleagues33 and Sarrias and colleagues38 showed reduced platelet serotonin levels in patients with depression, but no significant correlations between platelet serotonin levels and sex or age have been found in healthy donors.39,40 This independence of platelet serotonin levels from external parameters is advantageous for comparative studies and for general use as a clinical marker.
The overall hypothesis for this study was that platelet serotonin levels correlate with depression ratings for women with postpartum depression and reflect the response to treatment. If such a correlation could be demonstrated, platelet serotonin measures could aid in unbiased diagnosis, one of the greatest challenges in modern psychiatry. To test this hypothesis, we determined serotonin levels in platelets from patients with postpartum depression at 2 time points and compared them with the questionnaire outcomes.
Methods
The study included 13 patients (mean age 30.8, range 22–35 yr; 7 white, 2 South Asian, 2 First Nations, 1 Mexican and 1 Indo-Canadian) with postpartum depression according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), or similar criteria; only 11 women completed the study. Despite the DSM-IV criteria, postpartum depression is often clinically defined as an episode of major depressive disorder (MDD) occurring within 6 months after childbirth. Therefore, in the present study, we included women presenting with a diagnosis of MDD up to 6 months of giving birth. The protocol was approved by the Ethics Committees of the University of British Columbia and of St. Paul’s Hospital, Vancouver, and was conducted in accordance with the Declaration of Helsinki. Subjects gave written informed consent before each blood donation and confirmed that they did not take any medication known to interfere with platelet function for at least 2 weeks before donating blood. Subjects donated their first blood samples within 6 months of giving birth.
When the first blood sample was taken, every patient had a HAM-D score of 19 or higher. Patients 1–5 had acute onset of postpartum depression without prior pharmacological treatment, and patients 6–13 had not responded to a previous regimen of paroxetine treatment (patients 6, 7, 8 and 12 received 10 mg/d; patients 9, 10 and 13 received 20 mg/d; and patient 11 received 30 mg/d). Patients 12 and 13 dropped out of the study for nonmedical reasons. The second sample was donated approximately 8 weeks later, when patients 1–5 received paroxetine, and the treatment dosage for patients 6–11 was increased, as shown in Table 1. The treating physician monitored the patients for compliance on a weekly basis.
Summary of results comparing medication, HAM-D scores and platelet serotonin measures at first and second visit
Ten healthy female control donors (age 28–54 yr) participated in the study after providing written informed consent and confirmed that they had no medical condition and had not taken any medication for at least 2 weeks before blood donation.
Clinical procedures
HAM-D scores were assessed for every patient at the first visit and approximately 8 weeks later, at the second visit. Treatment responders were characterized by a 70% or greater reduction of their initial HAM-D score. According to this definition, patients 1 and 10 did not respond to their treatment. The serotonin levels were determined blind and were compared with the independently obtained HAM-D score at the end of the study.
Platelet preparation
We used platelet-rich plasma (PRP) in all experiments. Briefly, blood was drawn into sodium citrate (3.8% final concentration) and centrifuged at 150 g for 12 minutes at room temperature. PRP was removed, and aliquots were either fixed in paraformaldehyde (PFA; 2% final concentration in phosphate-buffered saline [PBS; 50 mmol/L NaH2PO4·H2O, 5 mmol/L KCl, 1.5 mmol/L MgCl2·6H2O, 80.1 mmol/L NaCl; pH 7.4]) or centrifuged at 1000 g for 15 minutes at 4°C to obtain platelet pellets for high-pressure liquid chromatography with electrochemical detection (HPLC-ECD). Fixation was carried out at room temperature for 45 minutes. All samples were frozen at –80°C until use.
Serotonin immunofluorescence and HPLC assay
Fluorescence and phase contrast microscopy were performed on a Zeiss Axioplan 2 microscope with a 100 ×/1.3 NA Plan Neofluar oil immersion objective and equipped with a digital camera (Digital Video Camera Company, Austin, Tex.). The immunocytochemical assay for microscopy and flow cytometry with the Epics XL flow cytometer (Beckman Coulter, Miami, Fla.) was described previously.34 Fixed platelets were permeabilized with Triton X-100 (0.2% final concentration) and washed with PBS before adding the monoclonal mouse antihuman serotonin antibody (Dako Diagnostics, Mississauga, Ont.). After incubation and another washing step, the secondary Alexa-488-labelled goat antimouse IgG1 (Cedarlane, Mississauga, Ont.) was added at a dilution of 1:40. Fluorescence and phase contrast microscopy were performed at the same time. Negative control samples for fluorescence microscopy were prepared as described above, except the incubation with the serotonin-specific antibody was omitted.
For automated, semiquantitative analysis by flow cytometry, labelled platelets as prepared for microscopy were diluted with PBS buffer 1:100 and analyzed with an Epics XL flow cytometer (Beckman Coulter, Miami, Fla.). The fluorescence resulting from the binding of fluorescently labelled nonspecific antibody alone was set to 2% platelet-associated fluorescence (negative control). Different sample aliquots from the same donation were analyzed in at least 3 independent experiments.
Serotonin concentrations in platelet pellets were measured with a Waters Alliance 2690 HPLC system in conjunction with an electrochemical detector (Waters, Alliance 2690–464), as previously described.33
Statistical analysis
We used post-analysis of variance (ANOVA) Newman-Keuls multiple comparison (t-test analysis, WINKS 4.80a software) to determine whether mean platelet serotonin levels as determined by flow cytometry were significantly different in healthy control subjects, compared with responding or nonresponding patients with depression.
Results
Platelet serotonin determination
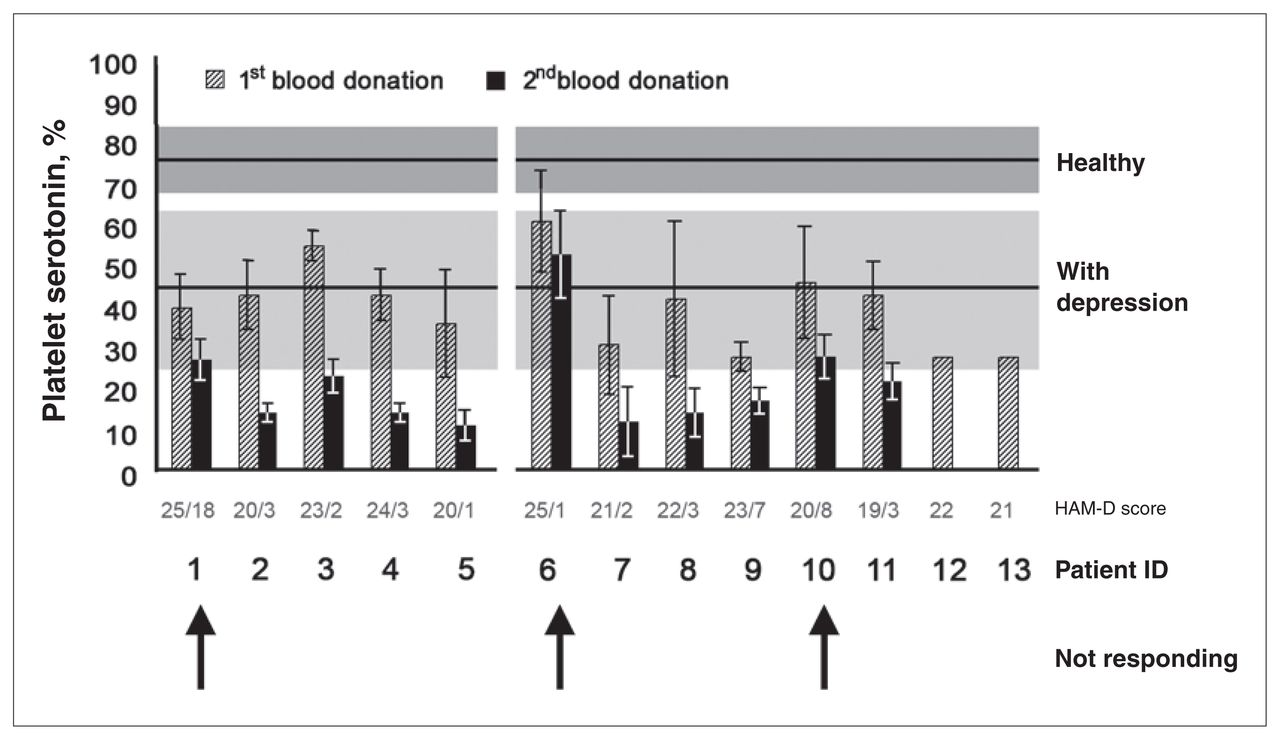
Irrespective of sex or age, the average platelet serotonin content in healthy control donors amounted to mean 884 (standard deviation [SD] 202) ng/109 platelets, which is equivalent to mean 78.3% (SD 8%) serotonin positivity of platelets measured by flow cytometry (Fig. 1). We calculated the percent of platelet serotonin by flow cytometry as the number of platelets that bind a specific antibody to serotonin in a total of 20 000 platelet counts. Samples taken from women with postpartum depression either before the start of treatment or not responsive to their initial treatment showed a significant reduction in the percent of platelet serotonin, to 45% (SD 11%) (Newman-Keuls multiple comparison, p < 0.001). This low serotonin level correlated with the serotonin content determined by HPLC-ECD, which averaged 406 (SD 311) ng/109 platelets. Table 1 summarizes the results of the first and second donation of blood samples by all of the women, except the 2 who did not complete the study.

Platelet associated serotonin. Platelet serotonin determined by flow cytometry (mean value and standard deviation [SD] from Table 1) in patients with postpartum depression, compared with normal and depression levels. The horizontal lines mark mean values with 1 SD depicted as boxes. Serotonin levels in the first blood samples were below normal, except patient 6 who, retrospectively, did not fit into the study, although she matched the study criteria. Patients 1, 6 and 10 did not respond to treatment (indicated by arrows).
For all 13 patients enrolled, ratings for depression (HAMD) were above 18 at the first visit (Table 1) and decreased in all women who responded to treatment, irrespective of whether they received paroxetine alone or paroxetine combined with cognitive–behavioural treatment. According to the definition of “responders” as women who showed a decrease in HAM-D score of at least 70% or greater, patients 1 and 10 did not respond to their treatment between the first and second visit. In line with the depression ratings, no significant treatment effect was seen from the flow cytometric serotonin determination in the platelets of these 2 patients (Fig. 1).
Platelet serotonin levels were not affected by the mean duration of the depressive episode before the first visit, which was, on average, 2.2 months. A minimum of 2 weeks is required for serotonin levels to stabilize during treatment, because this is the average turnaround time for platelets. The interval between the first and second visit was well above this limit, with a mean of 3.3 months. Similarly, discontinuation of treatment for 2 weeks would lead to a complete renewal of circulating platelets that have not been exposed to serotonin reuptake inhibitors. Therefore, platelet serotonin levels before treatment and after washout are expected to be equivalent. This was previously seen in patients with clinical depression (University of British Columbia, 2003. Unpublished data).
Comparable with the HAM-D scores, platelet serotonin levels were not related to the number of prior depressive episodes of patients (on average, they had 1 prior episode) or to the number of family members who also had depressive episodes. On average, our patients had 2 family members with clinical depression. Patient 6 showed very high serotonin levels in both blood samples, as measured with both flow cytometry and HPLC-ECD. According to the initial HAM-D score of 25, this patient was diagnosed with postpartum depression, not responding to 10 mg/day paroxetine. The second HAM-D score of only 1 suggested successful treatment with 20 mg/day paroxetine. We discuss the discrepancies of the depression ratings and the serotonin measures below, taking into consideration the special circumstances of this patient and highlighting the potential usefulness of objective measures for depression.
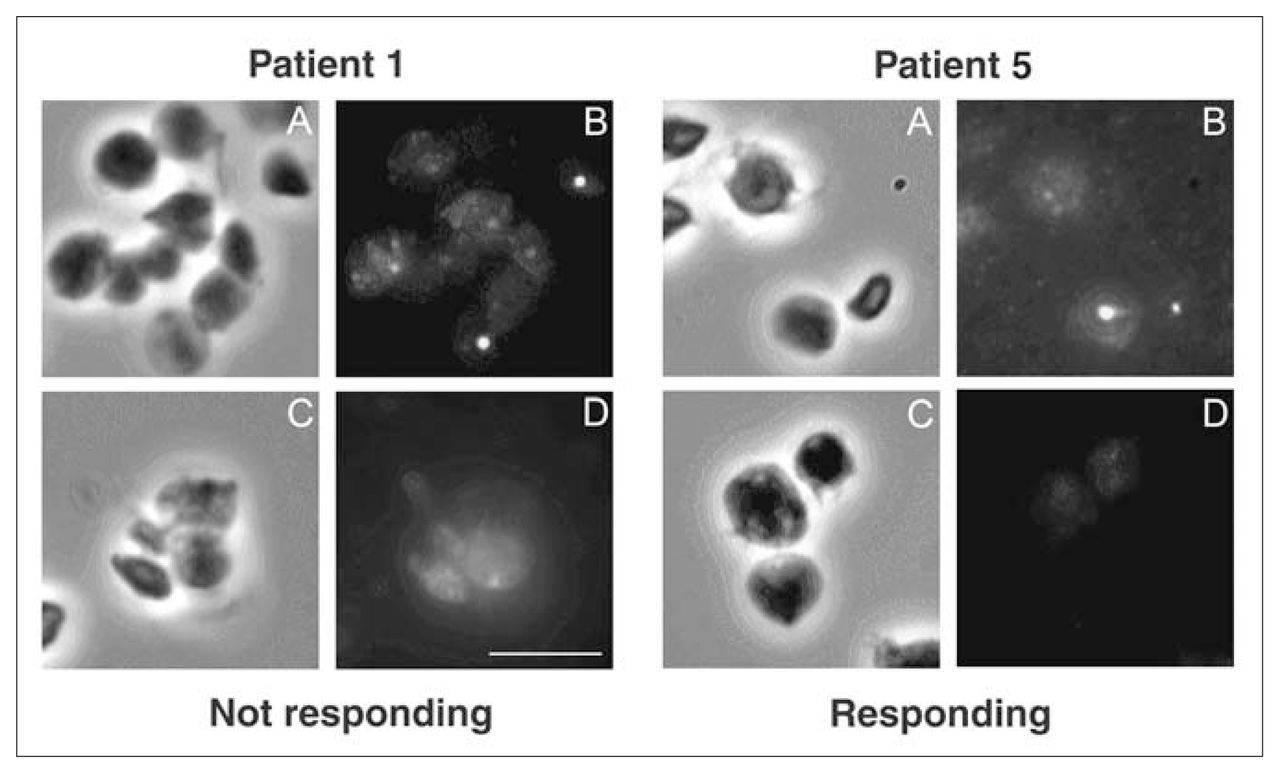
The number of platelets exhibiting bright green fluorescence from a binding of the specific serotonin antibody is automatically counted on the flow cytometer. The fluorescently labelled patients can also be manually enumerated on the microscope. Although the visualization on the microscope illustrates the validity of the flow cytometric assay, its time demand and subjectivity certainly precludes it as a routine test. As an example, Figure 2 shows representative micrographs of platelets at first (A,B) and second (C,D) visit from a patient who did not respond (patient 1) and a patient who did respond to treatment (patient 5). The nonresponding patient showed much higher serotonin labelling of platelets in the second sample (patient 1, D) than did the responding patient (patient 5, D). The percent of platelet serotonin obtained with flow cytometry and listed in Table 1 is the result of automated enumeration in a total of 2 × 104 platelets.

Immunocytochemical determination of platelet serotonin by microscopy. The micrographs shown are representative of samples from patients not responding and responding to treatment. Platelets from patients 1 and 5 were isolated from blood samples taken at the first (A, B) and second (C, D) visit and viewed with phase contrast (A, C) and fluorescence (B, D) microscopy. Several granules containing serotonin were visible in the first samples, because of the serotonin-specific green fluorescence labelling (B). These were also visible in the second sample (D) of nonresponding patient 1 but not in responding patient 5. The scale bar represents 5 μm.
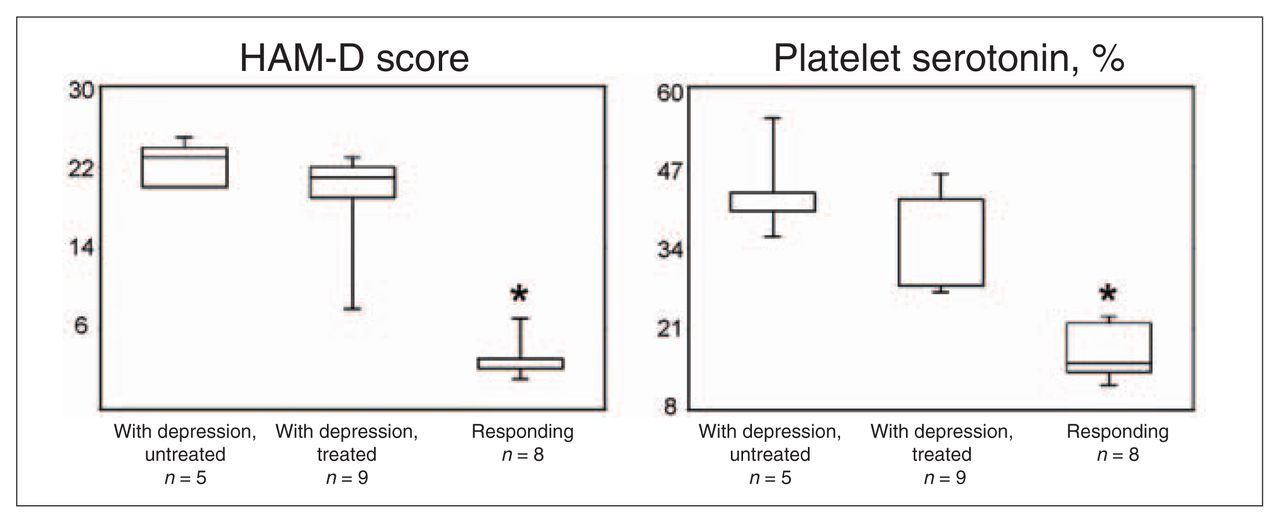
Newman-Keuls multiple comparison showed that mean platelet serotonin levels, as determined with the flow cytometry assay, were significantly lower in patients with depression than in healthy control subjects but were significantly higher in patients with depression who were untreated or nonresponding than in responders (p < 0.001 at the 0.05 significance level). HAM-D scores show the same statistical relation for these treatment groups (Fig. 3).

{kind=link}
{kind=link}
{kind=link}
Newman-Keuls multiple comparison block diagrams. Differences in mean Hamilton Depression Rating Scale scores and mean serotonin levels between 3 groups are shown: untreated depression patients (n = 5), treated but nonresponding and therefore still with depression (n = 9) and treatment responders (n = 8). Grouping was based on the results as shown in Fig. 1. Patient 6 was excluded. *p < 0.001.
Discussion
Our normal range of 884 (SD 202) ng/109 platelets, which is equivalent to 4.17 (SD 0.95) nmol/ 109 platelets considering a molecular weight of 212 g/mol for serotonin hydrochloride, corresponds well to literature values for a normal platelet serotonin content of 3.52 (SD 1.32) nmol/109 platelets.40 In another study, Flachaire and colleagues39 investigated 56 adults (26 women, 30 men; ages 28–58 yr) and observed normal serotonin concentrations of 3.81 (SD 0.87) nmol/109 platelets. Compared with this normal range of platelet serotonin that is unaffected by sex, age and time of day when the blood was collected,41 we found significantly lower platelet serotonin levels in women with postpartum depression. This agrees with our earlier finding that untreated major clinical depression, which was unrelated to childbirth, correlated with an approximately 50% reduction in platelet serotonin.33 Those results were obtained both with the flow cytometric serotonin assay as well as with the HPLC, a method previously used to detect reduced serotonin levels in MDD.
Patients with postpartum depression who were not responsive to their initial treatment also showed intermediate platelet serotonin levels. Responding patients were characterized by a severe serotonin deficiency with less than 22% serotonin-positive platelets. The results of Newman-Keuls multiple comparisons of HAM-D scores and serotonin content of platelets from the 3 treatment groups are shown in Figure 3. The results illustrate the significant difference between patients with depression before treatment or not responsive to treatment and patients who responded to treatment. As expected, the difference in HAM-D scores between untreated patients and patients who did not respond to treatment (treated depression patients) is not significant. A significantly reduced HAM-D score indicates treatment efficacy in patients who responded to treatment (p < 0.001). The comparison of platelet serotonin levels between the 3 treatment groups shows the same relation, that is, the serotonin levels in women who responded to treatment are significantly lower than in depression patients (p < 0.001). Data from all nonresponders were analyzed as one group because it is irrelevant whether the ineffective treatment was prescribed before or during the study. It can be assumed that patients who were already treated with paroxetine when they entered the study had slightly higher platelet serotonin levels before they started treatment. Because most patients receive treatment from their general practitioner before they see a psychiatrist, it is impossible and would be unethical to discontinue treatment for these patients to determine pretreatment platelet serotonin levels. In addition, the goals of this study were to determine whether platelet serotonin levels support the diagnosis of depression and are useful for identifying nonresponders, which we successfully demonstrated.
Interestingly, patient 6 showed relatively high serotonin levels throughout the study. We did not include these data in Figure 3. Her HAM-D scores suggested that she had depression while receiving treatment of 10 mg/day paroxetine and responded to an increased dosage of 20 mg/day paroxetine. However, her serotonin levels measured by flow cytometry and HPLC did not support the HAM-D scores. This woman’s history was characterized by severe psychosocial problems. Recovery from lifelong traumatic experiences is unlikely, and platelet serotonin levels suggested that paroxetine treatment was not truly effective in that patient. This particular case exemplifies how the platelet serotonin assay might be used as evidence-based support to optimize the care for women with postpartum depression.
Our findings are in line with recently published data showing increased serotonin reuptake inhibition in adolescents responding to SSRI treatment.15 Further, it has recently been shown that postpartum depression correlates with lower affinity of the platelet serotonin transporter (SERT) binding sites for [3H]paroxetine.21 The SERT is primarily responsible for serotonin uptake into platelets and, therefore, reduced affinity of the transporter for serotonin could explain the significantly reduced platelet serotonin levels among women with postpartum depression. In control subjects, Newport and colleagues21 showed that platelet serotonergic function is very stable over several weeks of the gestational (13.9–28.3 wk) and postpartum period (1.8–12.4 wk). Thus, it might be concluded that platelet serotonin levels do not significantly change during puerperium, despite changes in tryptophan metabolism.42 Studies measuring platelet serotonin levels as a function of time during gestation and puerperium are still needed.
Platelets represent a simplified, limited model for serotonergic neurons. However, SSRIs block the reuptake of serotonin into neurons and platelets by a comparable mechanism.13 Chemically, this means that successful treatment will lead to serotonin-depleted platelets. Consequently, serotonin is available outside the platelets. Its fate in plasma is unknown, whereas in the synaptic cleft, the prolonged presence of serotonin increases serotonergic signalling. We have not found increased levels of 5-hydroxyindole acetic acid (5-HIAA), the major metabolite of serotonin, in the urine of patients with depression, with or without treatment. This suggests that the body handles peripheral serotonin not just by rapid degradation and excretion. Another possible fate of peripheral serotonin could be its binding to a serotonin-binding protein, but the physiological consequences of such a mechanism are unclear.43,44
Generally, platelet serotonin levels measured with the immunocytochemical assay correlated well with the HPLC-ECD results. In some cases, there were minor differences between the 2 independent assays. It is possible that some platelet serotonin that can be detected by serotonin-specific antibody labelling does not yield to the quantitative determination by HPLC-ECD. The immunocytochemical assay is both easier to perform and also more meaningful for assessing postpartum depression.
Our results support the usefulness of platelet serotonin as a peripheral marker for postpartum depression and treatment response. In this preliminary study, we showed that platelet serotonin levels are significantly lower in women with postpartum depression, compared with healthy control subjects. Further, successful treatment with the SSRI paroxetine caused a reduction in serotonin-positive platelets below 25%. These results suggest that postpartum depression and treatment response affect platelet serotonin in a way similar to the effects of clinical depression unrelated to childbirth.33 However, the small sample size of our study is a limitation, and larger studies will be required to confirm our findings.
Acknowledgements
We thank all patients for their participation. We also thank Marsha MacDougall and Lisa Milis for technical assistance. This study was supported in part by Canadian Blood Services and by the Canadian Institutes of Health Research (MOP-61828).
Footnotes
Medical subject headings: serotonin; postpartum depression; paroxetine; selective serotonin reuptake inhibitors.
Competing interests: None declared for Drs. Maurer-Spurej and Pittendreigh. Dr. Misri has been a paid consultant to and received speaker fees from AstraZeneca, GlaxoSmithKline and Lundbeck.
Contributors: Drs. Maurer-Spurej and Misri designed the study and wrote the article. All authors acquired and analyzed the data, critically reviewed the article and gave final approval for its publication.
- Received April 22, 2006.
- Revision received June 11, 2006.
- Revision received September 9, 2006.
- Accepted September 11, 2006.