

Abstract
This paper describes a research program intended to provide a better understanding of the influence of several putative risk factors for schizophrenia on child development and psychosis. Two related components of the overall program are described: the retrospective EnviroGen projects, which use a variety of putative risk factors to explain variance in several dimensions of schizophrenia and in psychotic symptoms in community controls, and Project Ice Storm, which prospectively examines the effects of prenatal maternal stress in the children of women who were exposed to the 1998 Quebec ice storm during their pregnancies. The EnviroGen projects have been successful in explaining variance in several dimensions of illness, including premorbid adjustment and severity of dissociative symptoms. Project Ice Storm has demonstrated the noxious effects of prenatal stress on cognitive and language development in children. We have also found that “ice storm children” exposed in specific weeks of gestation show greater dermatoglyphic asymmetry, as has been reported for samples of patients with schizophrenia. In both studies, prenatal maternal stress has been associated with more severe childhood behaviour problems. The combination of retrospective and prospective studies is a rich source of triangulated results providing information about developmental psychopathology.
Introduction
The heterogeneity observed in schizophrenia is one of the most challenging aspects of this condition. Variability in symptomatology, course and outcome has led many researchers to suspect etiologic heterogeneity in schizophrenia.1 Despite a definite genetic component to schizophrenia, largescale epidemiologic studies have identified several non-genetic, environmental risk factors. However, the schizophrenia literature lacks studies that adequately test models of gene–environment interactions. As Malaspina et al2 wrote (p. 51), “research to date has supported the presence of gene–environment interactions in schizophrenia but has not allowed for any precise statements on the nature of this interaction. Chief among the limitations of this research were the reliance on imprecise data on both the genetic and environmental exposures and the inability to measure both exposures in the same individuals” [emphasis in original].
Testing gene–environment interactions is relatively new in psychiatry.3 Although recent reports have shown gene-by-environment effects in the development of depression in young people,4 little work has been done in this area for schizophrenia. Examining the associations among genetic and environmental risk factors for schizophrenia is the focus of our research program at the Douglas Hospital Research Centre in Montréal. We are conducting both retrospective studies of patients with schizophrenia and healthy adults (the EnviroGen projects) and prospective studies of children exposed in utero to various degrees of one particular risk factor for schizophrenia, prenatal maternal stress (Project Ice Storm). There are 3 main objectives of this research program: first, to increase understanding of how several putative risk factors for schizophrenia work individually and in combination to influence the risk for other putative risk factors; second, to understand how these risk factors influence development in several domains during childhood; and third, to understand how the risk factors explain variation in several dimensions of mental illness (rather than explaining risk for the illness itself). Integrated into the development of our research program are the concepts of gene–environment correlations and interactions, as described by several writers.2,3,5,6
Risk factors for schizophrenia
There is clearly a genetic component to schizophrenia. Heritability estimates average about 60%,7 although no genes have been reliably identified. The 50% concordance rate between monozygotic twins is striking evidence that this is a complex disorder involving genetic and nongenetic mechanisms. 8 Studies show that birth in winter,9 influenza in the mother during pregnancy,10 obstetric complications,11 childhood exposure to house cats and toxoplasmosis,12 and maternal exposure to a major stressor during pregnancy13 increase risk significantly, although with very modest effect sizes.14 Mednick et al15 hypothesized that it may be less the type of disruption of fetal development than the timing that is critical. Many studies of prenatal insults (e.g., stress, influenza) suggest that the worst outcomes are associated with stressors occurring at midgestation,16 a critical period for brain development. 17 Given a “progressive” view of neurodevelopment, 18 insults occurring during childhood and adolescence, such as abuse and neglect19 or drug abuse,20 may also disrupt neurodevelopment and predispose to mental illness.
Although several environmental risk factors have been shown to increase risk for schizophrenia, the magnitudes of these effects are small.14 Few studies, however, have examined multiple risk factors.21 Even fewer have explored associations among multiple risk factors, their timing and interactions, and dimensions of the illness itself. The EnviroGen projects are designed to address this gap. Given the great heterogeneity within the illness of schizophrenia, we are taking a dimensional, rather than categorical, approach, with the idea that factors increasing the risk for the diagnosis of schizophrenia by only a small magnitude may explain larger proportions of variance in specific dimensions of the illness.
The EnviroGen projects
We have developed a protocol for estimating the exposure of individuals to as many putative risk factors for schizophrenia as possible. Data are gathered from several sources. We conduct an interview with the patient’s mother to gather data on family history of mental illness, obstetric complications, prenatal stress, environmental exposures such as household and farm animals, premorbid adjustment, and the development of the patient’s illness. In an interview with the patient we gather data on his or her perspective on the history of illness onset, information on premorbid substance use, childhood abuse and neglect, other trauma in adulthood, symptom severity, minor physical anomalies and dermatoglyphics, and we collect blood samples for genotyping. From the patient’s obstetric and psychiatric hospital charts we gather data on the patient’s birth, as well as indices of illness onset and response to pharmacologic treatment. Using databases from Environment Canada we calculate exposure to temperatures and sunlight hours for each week of pregnancy. Similarly, using a Health Canada database we estimate risk of exposure to respiratory infections during each week of pregnancy according to the recorded number of deaths due to pneumonia and influenza in Montréal.
Our pilot study, with more than 40 patients to date, demonstrates the feasibility of these methods. We are now collecting data on an additional 120 patients, the majority of whom have been recruited through the recently founded Program for the Evaluation and Prevention of Psychosis (PEPP Montréal) first-episode psychosis clinic to ensure more reliable retrospective reports and to provide a more representative sample. To provide a control group for the EnviroGen sample, we are applying the EnviroGen protocol to 120 community controls (matched for age, sex and education) selected from a sample of 2400 subjects who responded to a screening questionnaire. We are also running a project related to the association between schizophrenia and post-traumatic stress disorder (PTSD), as described below.
Our first objective in the EnviroGen program is to understand associations among risk factors and to uncover gene-by-environment (G×E) and environment-by-environment (E×E) correlations. For this objective, we are guided by Kraemer et al,3 who distinguished among 5 types of associations between risk factors as they relate either to a more distal risk factor or to an outcome. As a function of temporal precedence, intercorrelation and dominance (i.e., the relative strengths of their correlations with the third variable), 2 risk factors may qualify as either independent, overlapping or proxy risk factors and may relate in a mediating and/or moderating fashion with the third variable. In our larger sample of patients with psychosis, we will determine the specific nature of associations among the risk factors.3 We will pay special attention to the possibilities of mediating effects (i.e., that risk factor A may increase the risk for factor B, which then increases the risk for the outcome variable) and especially moderating effects (i.e., that the effect of factor A on outcome is limited to individuals with a particular value for factor B).
Preliminary results from EnviroGen22 suggest that family history of schizophrenia and the nongenetic risk factors are not independent and that there are 2 main trajectories: in the first, a positive family history of schizophrenia increases risk for prenatal stress (r = 0.406), obstetric complications (r = 0.355) and childhood maltreatment (r = 0.603); in the second, winter birth is associated with premorbid substance use, especially in cases without a family history (r = 0.500).
Using the dichotomous variable for family history of psychosis, we have already found a number of situations in which family history moderates the association between an environmental risk factor and outcome. In an example of gene–environment interaction, the pilot data suggest that family history moderates the effect of childhood maltreatment on response to antipsychotic treatment.23 Family history of mental illness is, admittedly, a proxy variable for genetic loading or possibly for a specific genotype. In the upcoming year, we will be testing associations between each risk factor and several genotypes that one of us (R.J.) has found to be associated with response to antipsychotic treatment24 including catechol-O-methyl-transferase (COMT). Using more refined genotype data, we anticipate uncovering G×E interactions similar to those found by Caspi et al4 in a study of the Dunedin cohort: among 26-year-olds, a greater number of life events (or more serious childhood maltreatment) were associated with more severe depression, but only in subjects with 1 or 2 copies of the short allele of the serotonin transporter promoter polymorphism. More recently, the Dunedin project uncovered an important interaction between COMT genotype and cannabis use in adolescence such that the combination of cannabis use and having 2 copies of the valine (Val) allele of COMT increases risk for schizophrenia spectrum disorders by a factor of 10.25 We may similarly find that certain genotypes moderate the effects of nongenetic risk factors on the severity of particular dimensions of psychotic illness.
Although the results for patients are interesting, they may not reflect associations among risk factors in the nonpsychiatric population. For example, the literature suggests that childhood trauma predicts substance use,26 but in our patients we found a strong negative association.22 By the end of 2005 we will have conducted analyses of associations among genetic and environmental risk factors for the 120 controls.
With regard to the second objective, which is to test the associations between our set of putative risk factors for schizophrenia and child development, results to date suggest that the worst adjustment in several domains of the retrospective Child Behaviour Checklist is associated with a combination of positive family history of schizophrenia and nonwinter birth27 (Fig. 1). In addition, prenatal stress in the pilot sample was associated with more severe externalizing problems on the retrospective Child Behaviour Checklist (unpublished observation).

Rates of childhood attention problems as reported by mothers of patients with schizophrenia born in winter (December– March) or nonwinter months, with (squares) or without (circles) a family history of schizophrenia. Reproduced from St-Hilaire et al27 (Schizophr Res 2005;73:39–48).
Our third objective is to determine the associations between risk factors and dimensions of illness. In analyses to date, we explained 46% of the variance in duration of untreated psychosis as a function of family history, premorbid internalizing problems and age at onset of the psychosis.28 The data also suggest that we can explain up to 55% of the variance in some of the core symptoms of schizophrenia using various combinations of risk factors (unpublished observation). Reported emotional abuse alone explained 70% of the variance in dissociative symptoms,29 which are common in schizophrenia.
To investigate the role of childhood maltreatment more closely, an EnviroGen spin-off project is testing the hypothesis that part of the heterogeneity of schizophrenia may be due to confounding with PTSD. PTSD has many of the same symptoms as schizophrenia, and many patients with schizophrenia have psychophysiologic characteristics typical of PTSD.30 Patients with severe mental illness have high rates of exposure to trauma31 and PTSD.32 The goal of the PTSD addendum to EnviroGen is to understand the role of trauma, in combination with other genetic and environmental risk factors, in explaining the wide variation among patients with schizophrenia in several psychophysiologic domains: diurnal patterns of cortisol secretion, event-related potentials (P300), startle response (prepulse inhibition) and stress reactivity as reflected in cortisol changes. Data from our first 14 subjects demonstrate that patients with self-reported childhood trauma have significantly lower morning cortisol secretion33 (Fig. 2), as is seen in people with PTSD,34 which suggests that this line of research is promising.
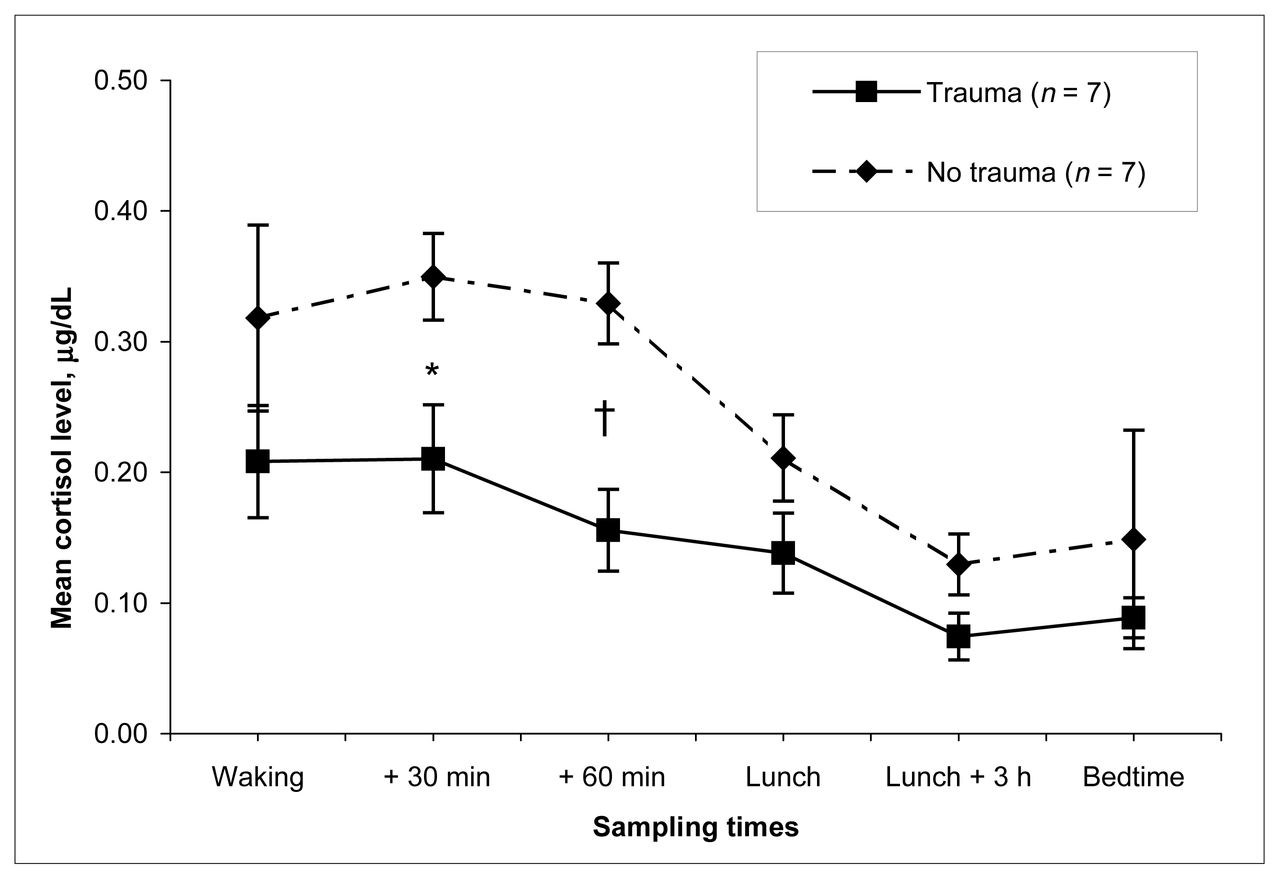
Mean (and standard error of the mean) salivary cortisol levels in patients with schizophrenia as a function of childhood trauma group and time of collection. Intervals between sampling times are not scaled equally. *Significant at the 0.05 level (2-tailed); †significant at the 0.01 level (2-tailed). Reproduced from Braehler et al33 (Schizophr Res, in press).
In the EnviroGen community control replication, 2400 adults were approached in public areas in Montréal and were asked to complete the brief Community Assessment of Psychic Experiences (CAPE),35 which assesses psychotic, negative and depressive symptoms. We included in our analyses adults between the ages of 18 and 40 and excluded subjects who indicated that they had taken prescription antipsychotic medication (among a long list of medication names) at any time in their lives. In the original Dutch studies with the CAPE, 17%–20% of the sample admitted to experiencing at least 1 of several severe psychotic symptoms, and we obtained similar results in Montréal.36 Our questionnaire also included several items about nonthreatening risk factors, analyses of which show significant associations between higher CAPE psychotic symptom scores and winter birth, a history of head trauma, more house moves during childhood and exposure to housecats during childhood. There was no association between CAPE scores and parental age. With the extensive risk factor data obtained during the EnviroGen testing of 120 of these subjects, we will test the explanatory value of more important risk factors such as family history of mental illness and childhood trauma. With this sample, we will also test the roles of the same mediating, moderating and outcome variables that we are assessing in patients. Most important, we will be able to determine whether the severity of psychotic-like symptoms experienced in a community sample can be explained by the same risk factors that explain variance in psychotic symptoms in a clinical sample. Thus, our results will add data to the debate on whether psychotic illnesses like schizophrenia lie at one end of a broad continuum or whether the differences between clinical and nonclinical levels of psychosis are more qualitative than quantitative.
Project Ice Storm
Prenatal maternal stress (PNMS) is a significant risk factor for schizophrenia, as demonstrated by large, retrospective epidemiologic studies.16 Despite considerable research with rodents, primates and humans, the mechanisms responsible for the association between PNMS and schizophrenia are unclear because of methodologic limitations that we have elaborated elsewhere.37
We have taken advantage of a natural disaster to overcome many of the shortcomings in the human prenatal stress literature. In January 1998, southern Quebec received 5 days of freezing rain that left 3 million people without power for as long as 40 days during the coldest months of the year. In June 1998, we recruited 224 women who had been pregnant during the crisis or who became pregnant within 3 months after the crisis. Our surveys teased apart their “objective” stress exposure (e.g., days without power) from their “subjective” reactions (e.g., post-traumatic stress symptoms) and physiologic reactions (7 samples of salivary cortisol over 24 hours). A series of follow-up assessments have occurred since the infants were 6 months old, a postal questionnaire is currently in process with the children at 6½ years of age, and other face-to-face and postal assessments are planned for the next 3 years.
The advantages of Project Ice Storm are the “independence” of the stressor; the great variation in both the severity of exposure and timing relative to pregnancy among the subjects; the possibility of separating objective hardship, subjective stress and physiologic stress response; the large number of pregnant women who were exposed; and the ability to assess exposure and its effects soon after they occurred and to follow the offspring prospectively.
With respect to the first objective of our research program, which is to determine the associations among risk factors for schizophrenia, our results to date from Project Ice Storm have already demonstrated that PNMS from the ice storm predicts other outcomes known to be risk factors for schizophrenia, such as prematurity, being in an incubator as a newborn and obstetric complications.
We have also demonstrated that the timing of PNMS is associated with a biological marker of schizophrenia, dermatoglyphic asymmetry.36 It has been found that patients with schizophrenia have, on average, greater asymmetry between homologous fingers in the number of ridges between certain landmarks on the fingerprints.38 There is considerable debate as to whether this finding reflects genetic or environmental factors.38 Although Newell-Morris et al39 found greater dermatoglyphic asymmetry in macaque infants whose mothers had been stressed during pregnancy, ours is the first demonstration of this effect in humans: children whose mothers were without electricity for any length of time between gestational weeks 14 and 22 had significantly greater asymmetry than other ice storm children, an effect that was greatest in those whose mothers also experienced a high degree of subjective distress related to the ice storm.
As for increasing our understanding of the associations between risk factors and child development, the second objective of our program, our Project Ice Storm results demonstrate strong effects of PNMS on outcomes in infants and toddlers: when a subset of children were tested with the Bayley Scales of Infant Development at 2 years of age, those whose mothers had experienced moderate or high levels of ice storm stress (objective) had significantly lower Mental Development Index scores (analogous to IQ [intelligence quotient]) than the low stress group (p < 0.01),40 corresponding to two-thirds of a standard deviation difference (Fig. 3). This effect was seen in those exposed to the ice storm during the first or second trimester. The group with high objective stress also had lower receptive (p < 0.05) and expressive (p < 0.01) vocabularies.40 Although the Bayley Scales of Infant Development, used to assess general intellectual functioning at age 2, do not separate scores into verbal and nonverbal components, the magnitude of the effect on the vocabulary scores from the MacArthur Communicative Development Inventory leads us to suspect that the bulk of the effect of the PNMS is on language development. The next challenge is to determine the extent to which these effects remain with increasing age. Our evaluations of the children at age 5½ years suggested that the effects of PNMS on cognitive development endure at least into kindergarten.

Scores on the mental development index (MDI) of the Bayley Scales of Infant Development for children in high (solid bars) or low (open bars) objective stress groups, exposed to the ice storm in the first, second or third trimester. Data source: Laplante et al.40
Project Ice Storm also responds to our goal of understanding the associations between risk factors for schizophrenia, especially PNMS, and dimensions of psychiatric symptoms, the third program objective. When the ice storm children were 3½ years of age, the parents completed the Child Behaviour Checklist. The results suggest that the degree of PNMS explained 28%–30% of the variance in children’s internalizing and externalizing problems, even after adjustment for maternal psychopathology.
The mechanisms responsible for these effects on child development have not yet been uncovered within the context of Project Ice Storm. Results from animal research suggest that the fetuses of stressed dams are the victims of surges in maternal glucocorticoids.13 Yet our study suggests that there is only a modest correlation between the severity of objective stress exposure and subjective stress reactions among “ice storm mothers,” and that these subjective stress reactions are then associated with lower, not higher, basal cortisol in the mothers. In addition, the greatest dermatoglyphic asymmetry in the children (presumed to reflect prenatal developmental insult) is associated with lower, not higher, maternal cortisol. Other research programs with rodents suggest that maternal behaviours can be responsible for altered stress reactivity in the offspring.41 Research with nonhuman primates, however, shows that pregnancy stress does not alter maternal behaviours despite significant effects on infant development.42 Given that our cortisol data were collected 5–6 months after the end of the ice storm crisis, Project Ice Storm is not ideal for studying the role of maternal stress hormones in affecting child development. Future disaster studies will be better positioned to collect more timely samples of maternal hormones and to test the hypothesis of epigenetic programming by maternal behaviours.
Conclusions
Rutter called for an “explicit research focus on the forms of interplay between genes and environment” (p. 390).6 Our research program has been designed to meet that challenge, and results to date are beginning to describe the nature of these interactions. Our approach is likely to give us a more complete and accurate picture of how risk factors for schizophrenia work together to explain variance in different dimensions of human development than has been achieved to date. Combining the retrospective approach of EnviroGen with the prospective Project Ice Storm provides a triangulation of results: as we find, for example, that patients with schizophrenia who have a history of prenatal maternal stress had more severe externalizing problems as children, we can immediately test out this hypothesis prospectively in Project Ice Storm children (for whom, indeed, greater stress predicts more severe externalizing problems in childhood). In fact, we see many patterns developing in the ice storm cohort that are well-known characteristics of children at high risk for schizophrenia: 43 poorer IQ and language development, more internalizing problems, poorer balance, dermatoglyphic asymmetries and others. Thus, while the literature on risk factors for schizophrenia prompted initiation of Project Ice Storm, this prospective study validates many of the findings from the retrospective EnviroGen project, at least concerning one risk factor for schizophrenia, that being prenatal maternal stress. Our ultimate goal will be to use the findings from both projects to build developmental models of several dimensions of psychopathology.
Acknowledgements
We thank all of the research assistants, interviewers and students who have worked on the EnviroGen and Ice Storm projects, as well as the subjects who have graciously participated. Dr. King’s work has been supported by research fellowships from the Fonds de recherche en santé du Québec (FRSQ). The EnviroGen project has been funded by grants to Dr. King from the FRSQ and from the Schizophrenia Axis of the FRSQ Mental Health Network. Project Ice Storm has been supported by grants from the McGill University Stairs Memorial Fund, the Canadian Psychiatric Research Foundation, and the Canadian Institutes of Health Research to Dr. King and by a grant from the Schizophrenia Axis of the FRSQ Mental Health Network to Dr. Laplante.
Footnotes
Medical subject headings: schizophrenia; stress, psychological; child development; prenatal development; risk factors.
Competing interests: None declared.
Contributors: Dr. King conceived of and designed the study and acquired and analyzed data. Dr. Laplante collected and analyzed data for Project Ice Storm. Drs. King and Joober drafted and revised the article. All authors approved the final version to be published.
- Received February 17, 2005.
- Revision received June 22, 2005.
- Accepted July 4, 2005.
References

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.