

Abstract
Objective: Recent functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) studies based on the symptom provocation paradigm have explored neural correlates of the cognitive and emotional processes associated with the emergence of obsessive–compulsive disorder (OCD) symptoms. Although most studies showed the involvement of cortico–subcortical loops originating in the orbitofrontal cortex and the anterior cingulate cortex, an increased activity within numerous other regions of the brain has inconsistently been reported across studies. To provide a quantitative estimation of the cerebral activation patterns related to the performance of the symptom provocation task by OCD patients, we conducted a voxel-based meta-analysis.
Methods: We searched the PubMed and MEDLINE databases for studies that used fMRI and PET and that were based on the symptom provocation paradigm. We entered data into a paradigm-driven activation likelihood estimation meta-analysis.
Results: We found significant likelihoods of activation in cortical and subcortical regions of the orbitofrontal and anterior cingulate loops. The left dorsal frontoparietal network, including the dorsolateral prefrontal cortex and precuneus, and the left superior temporal gyrus also demonstrated significant likelihoods of activation.
Conclusion: Consistent results across functional neuroimaging studies suggest that the orbitofrontal and anterior cingulate cortices are involved in the mediation of obsessive–compulsive symptoms. Based on recent literature, we suggest that activations within the dorsal frontoparietal network might be related to patients’ efforts to resist the obsessive processes induced by the provocation task. Further research should elucidate the specific neural correlates of the various cognitive and emotional functions altered in OCD.
Introduction
Obsessive–compulsive disorder (OCD) is a chronic and highly disabling condition that affects 2%–3% of the general population. This anxiety disorder is characterized by the presence of obsession in the form of intrusive and distressing thoughts, ideas or images, and by the urge to perform repetitive or ritualistic behaviours known as compulsions.1,2 It has been proposed that obsessions are related to the increased evaluation of negative consequences following an action that an individual with OCD wrongly interprets as erroneous or faulty. This persistent high “error signal,” which is considered to be the core of OCD symptomatology, may initiate the pathological doubt that is usually associated with increased anxiety.2–5 Compulsions may then occur as behavioural outputs aiming to relieve or to neutralize the anxiety induced by the obsessional process. The relief that may be equated with a form of reward is only transient because performed behaviours do not definitively stop the “error signal,” which leads to a cyclic reproduction of these behaviours.2 This phenomenologic view suggests that several cognitive processes such as error detection, together with emotional and motivational functions, may be altered in OCD.2,5
Remarkable advances in functional neuroimaging have recently provided results that showed the participation of several regions of the brain in the cognitive and emotional processes altered in OCD, and their overactivity in patients with the disorder.2,6 Indeed, most neuroimaging studies have reported an increased functional activity in the cortico–striato–pallido–thalamo–cortical circuits originating within both the orbitofrontal and the anterior cingulate cortices in OCD patients compared with individuals without the disorder. Furthermore, this basal cortico–subcortical overactivity may be reduced in conjunction with the clinical improvement obtained with efficient treatment.2,7 A recent meta-analysis based on the calculation of regional effect sizes across neuroimaging studies that compared functional activity in patients with OCD and healthy individuals found consistent and significant changes in the left orbitofrontal cortex and bilateral caudate nucleus.8 However, a meta-analysis using the activation likelihood estimation method may provide further insight, especially regarding the possible roles of other regions of the brain in the pathophysiology of OCD. Voxel-based analysis, which allows a high spatial level of distinction, quantitatively evaluates converging activation foci across functional imaging studies by modelling each activation focus as the centre of a normal probability distribution.9 Moreover, recent neuroimaging studies involving patients with OCD have focused on the symptom provocation task, which entails the presentation of obsessional stimuli leading to the production of OCD symptoms. Such experimental protocols seem to be more relevant to elicit neural patterns of activations related to the emergence of obsessive–compulsive symptoms than paradigms based on measuring functional activity during a “resting state.” We conducted a paradigm-driven meta-analysis using the activation likelihood estimation method to provide a complete overview of the cerebral networks activated during the symptom provocation task in patients with OCD.
Methods
Literature search and study selection
We searched the PubMed and MEDLINE databases for studies that used functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) to examine brain activity during a symptom provocation task in patients with OCD. Our keywords for the literature search included “obsessive–compulsive disorder” and any of the following terms: “functional magnetic resonance imaging,” “positron emission tomography” and “symptom provocation task.” To obtain additional papers, we manually searched the reference lists of the studies we retrieved.
We included studies in our analysis if they were published in English in a peer-reviewed journal, were restricted to fMRI and PET (C15O2, H215O and 15O2) scanning techniques that measure highly interrelated biological phenomena,10 included patients with a primary diagnosis of OCD, were based on a symptom provocation paradigm involving the presentation of obsessional stimuli, described activations at a conventional level of significance and reported the coordinates of activation maxima in a standardized stereotactic space.
One author (J.-Y.R.) identified all articles (n = 8)11–18 that were published before July 2007 and met our inclusion criteria. Another (B.A.) independently verified and confirmed the study selection.
Data abstraction, coding and correction
We abstracted the coordinates and the volumes of each of 102 activation foci and the corresponding statistical values from conditional contrasts (“symptom provocation condition” minus “neutral condition”). We entered the data into Submit software (BrainMap, University of Texas).19 Because data on conditional contrasts were unavailable for patients with OCD in the study by Mataix-Cols and colleagues, we considered the between-group contrast (“patients with OCD” minus “individuals without OCD”).15 To renormalize coordinates spatially into a single stereotactic space, we converted Montréal Neurological Institute coordinates to Talairach coordinates using Brett transformation.20,21 In Talairach space, the x coordinate corresponds to the lateromedial distance, the y coordinate to the anteroposterior distance and the z coordinate to the superoinferior distance from the anterior commissure. We reported activation extents in cubic millimetres. We calculated voxel size when appropriate using Equation 1.

We inserted the statistical values (t statistics or z scores) corresponding to the maximum or to the mean activation focus in the analysis when available.
Activation likelihood estimation
We completed our activation likelihood estimation using Search&View software (BrainMap, University of Texas).19,22,23 We divided the Talairach space into 2 × 2 × 2-mm voxels. Activation foci were modelled by a 3-dimensional normal function with a full width half maximum of 10 mm. We used a permutation test of randomly distributed foci to determine the statistical significance of the resulting activation likelihood estimation values. We performed 5000 permutations with the same full width half maximum value and the same number of foci that we used to compute the activation likelihood estimation values. We then corrected the permutation test for multiple comparisons by using the false discovery rate method.24 We used a statistical threshold of p < 0.01 for the generated activation likelihood estimation map, and we did not select a minimum cluster size. We used AFNI software to visualize the activation likelihood estimation map overlaid onto a high-resolution brain template generated by the International Consortium for Brain Mapping.25,26
Results
Study selection
We included 8 studies in our meta-analysis (Table 1). Their main results are summarized in Table 2. Of the 8 original studies, 3 studies included patients who received selective serotonin reuptake inhibitor or clomipramin therapy.13,15,16 The study by Mataix-Cols and colleagues15 included patients prescribed additional medications: buspirone (n = 3), lithium carbonate (n = 1), valproate sodium (n = 1) and chlorpromazine (n = 1).
Functional neuroimaging studies included in the meta-analysis
Locations of the main activations reported in the 8 functional neuroimaging studies included in the meta-analysis
Activation likelihood estimation
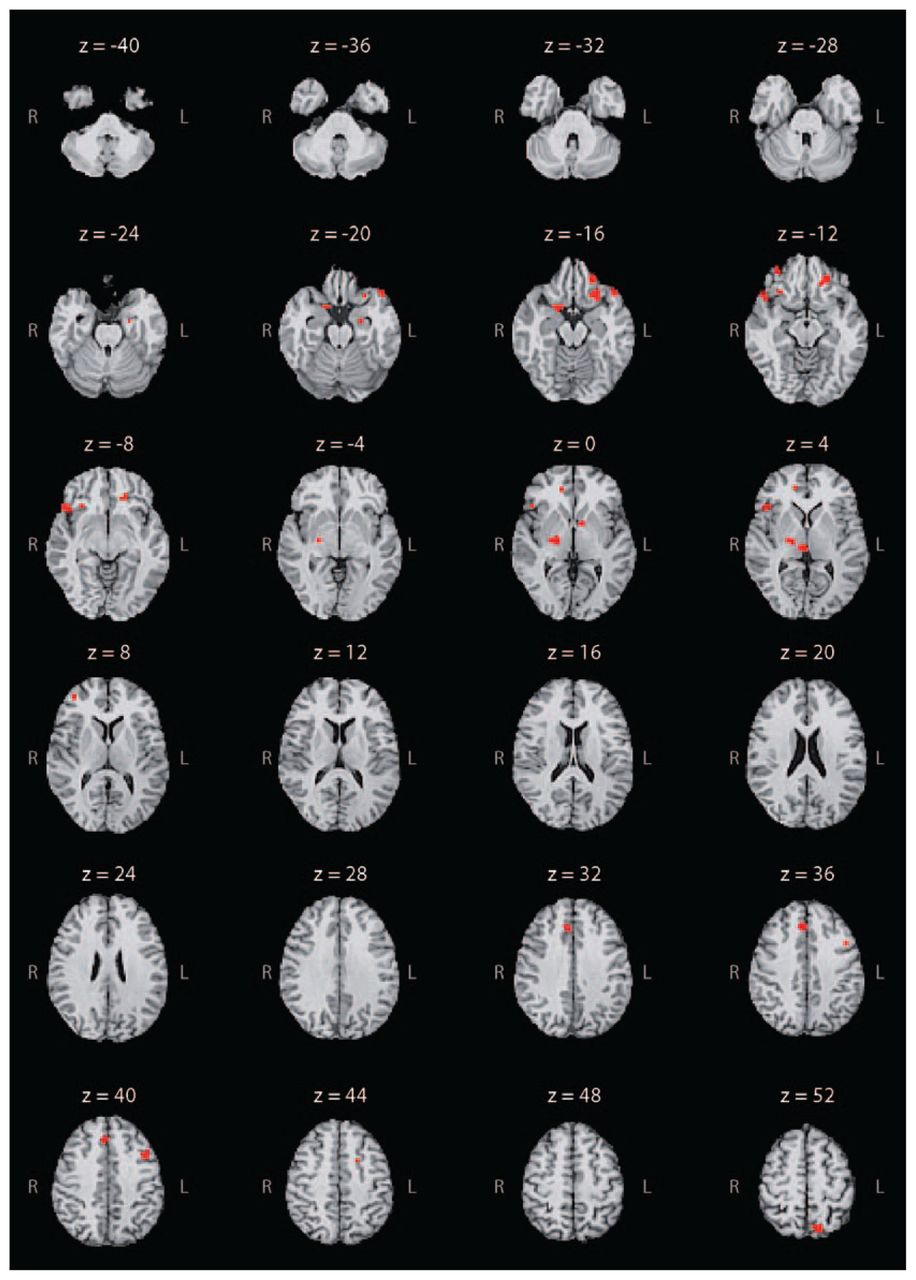
Results of our activation likelihood estimation based on the provocation of OCD symptoms revealed 19 clusters of significant likelihood for activation. We found significant likelihoods of activation in several cortical regions, including the bilateral orbitofrontal cortex (Brodmann areas [BA] 11, 45, 47), right anterior prefrontal cortex (BA 10), bilateral anterior cingulate cortex (BA 24, 32), left dorsolateral prefrontal cortex (BA 9), left precuneus (BA 7), right premotor cortex (BA 6) and the left superior temporal gyrus (BA 38). In addition, we detected significant likelihoods of activation in the bilateral external globus pallidus, the left hippocampus and in the right uncus. The coordinates, the activation likelihood estimation value and the volume of each cluster are reported in Table 3. Locations demonstrating significant likelihoods of activation are depicted in Figure 1.

Meta-analytic activation map based on symptom provocation studies involving patients with obsessive–compulsive disorder. Regions of the brain showing a significant activation likelihood are highlighted in red on axial slices of an individual brain in the Talairach space. They include the bilateral middle and inferior frontal gyri (z = −16, −12, −8), bilateral cingulate cortex (z = 0, 4, 44), bilateral globus pallidus (z = −4, 0, 4), left hippocampus (z = −24) and right uncus (z = −20). We obtained a unilateral significant threshold in the superior temporal gyrus (z = −20, −16) and precuneus (z = 52) for the left hemisphere, and in the medial frontal gyrus (z = 40) and thalamus (z = 4) for the right hemisphere.
Clusters of significant likelihood for activation based on activation likelihood estimation
Because we used between-group contrasts from Mataix-Cols and colleagues,15 we conducted a sensitivity analysis with and without the inclusion of these data to assess the stability of our results. We found no marked differences regarding cerebral regions that demonstrated significant likelihoods of activation with the inclusion of foci reported in this study. However, additional cerebral regions demonstrated significant likelihoods of activation in the analysis without foci from Mataix-Cols and colleagues, including the right insula (BA 13; x = 44, y = 0, z = 6), left caudate (x = −12, y = 12, z = 10), right posterior cingulate (BA 29; x = 12, y = −42, z = 12) and right superior parietal lobule (BA 7; x = 28, y = −64, z = 46). The corresponding volume for each of these regions was inferior to 10 mm3.
Discussion
A paradigm-driven meta-analysis provides a quantitative estimation of the convergence of activated cerebral regions during the performance of a given paradigm by a given population. Thus a meta-analysis using the activation likelihood estimation method should contribute to elucidating the neural mechanisms underlying pathological processes such as those involved in the production of obsessive–compulsive symptoms. Our study confirmed the importance of well-known cortico–striato–pallido–thalamo–cortical circuits that have been shown to be overactive in OCD. Our study also highlighted the involvement of other cerebral structures in the performance of a symptom provocation task. We found a significant likelihood of activation within frontosubcortical loops with high concordance across included studies. We also found significant results in unexpected regions of the brain, such as the temporal and parietal cortices.
The orbitofrontal cortex is commonly distinguished by its medial and lateral parts.27 The medial region extensively connects with the paralimbic–limbic system, including the insular cortex, cingulate gyrus, amygdala and hypothalamus.27–30 This area is highly involved in encoding the representation of the value of an expected outcome, which is used to anticipate the positive and negative consequences that are likely to follow a given action.28,30 The lateral orbital region is more connected to higher neocortical systems, particularly the dorsolateral prefrontal cortex. The lateral orbital region is thought to play a role in several cognitive processes, such as the selection, comparison and judgment of environmental stimuli, but also in the monitoring of error recognition.29,30 These orbitofrontal regions, which are known to be overactive in patients with OCD, might contribute to an increased evaluation of the occurrence of negative consequences following an action.2,8 This phenomenon might generate obsessive thoughts that lead to repetitive or ritualistic behaviours intended to prevent negative consequences as a way to relieve anxiety.2
Different versions of the Stroop paradigm have largely contributed to distinguishing a cognitive division (the most dorsal part) and an affective division (the most ventral part) of the anterior cingulate cortex.31,32 Several neuroimaging studies have shown that the cognitive division is involved in monitoring conflict and detecting error, whereas the affective division is involved in processing emotion, including the assessment of emotional information and the regulation of emotional responses.32 The cognitive division has extensive connections with the dorsolateral prefrontal and the parietal cortices, as well as with the primary, premotor and supplementary motor areas. The affective division projects more directly to the orbitofrontal cortex, amygdala, nucleus accumbens, hypothalamus and hippocampus, which demonstrated a significant likelihood of activation in our analysis.33 Over-activity in the cognitive division, as observed in patients with OCD, may be involved in the dysfunctional monitoring of high-conflict situations, placing the patient in a potential position to make an error. Overactivity may also be involved in the increased evaluation among patients with OCD of actions they wrongly interpret as erroneous or faulty.2,34,35 Therefore, the cognitive division seems to be involved in the generation of the high “error signal” that is considered to be the core of OCD symptomatology. On the other hand, because of its closed connections with the limbic system, the affective division might mediate the clinical expression of anxiety symptoms associated with the obsessional process.2–5
The orbitofrontal and anterior cingulate cortices have strong connections through the ventral striatum, the pallidum and the medial thalamus. The different levels of these cortico–subcortical loops are thought to be involved in the pathogenesis of OCD. According to our results, the external globus pallidus might play a direct role in the production of obsessive–compulsive symptoms; however, the mechanisms by which it contributes to the emergence of these symptoms remain a matter of debate. It has been reported that OCD symptoms occur following pallidal lesions; however, microinjections of a GABAergic antagonist in monkeys induced overactivity in the limbic part of the external globus pallidus, causing the monkeys to repeat particular behaviours.36–38 This apparent discrepancy could be related to the precise regions of the external globus pallidus that might be more directly involved in OCD. Our results showed no significant likelihood of activation in the ventral striatum, which is considered to be a crossroads where cognitive, emotional and motivational information abounds via its multiple connections within the frontosubcortical loops. However, there are strong arguments in the literature for considering the striatum, especially the caudate nucleus and nucleus accumbens, to be involved in the mediation of OCD symptoms.
In another study, our research team found that neuronal activity in the caudate nucleus differed according to the presence of OCD symptoms.39 We found an increase in firing rates and neuronal irregularities in 2 of 3 patients with OCD who had surgery for deep brain stimulation. Both patients experienced obsessions during the neuronal recordings.39 Furthermore, several studies have reported the efficacy of deep brain stimulation with the striatal region as a surgical target among patients with OCD that is resistant to treatment. 40–44 The main reason for the lack of striatal activation in our present meta-analysis could be our choice of a conservative threshold of α = 0.01 to minimize type I error. Among the 8 studies included in our analysis, 4 demonstrated activation within the right striatum and 2 demonstrated activation in the left striatum (Table 2). When we applied a less conservative threshold of α = 0.05, we identified additional regions, including the caudate nucleus (3 foci, x, y, z: 12, −4, 20; 8, 0, 8; −12, 12, 10). Because the number of foci varied across the studies (owing to heterogeneity of experimental procedures) and because the activation likelihood estimation method attributed equal weight to the findings of each study, it seemed advisable to use a conservative threshold to identify the regions of the brain most commonly involved in the performance of the OCD symptom provocation task.
The significance of the likelihood activation that we observed in the left-sided superior temporal gyrus, precuneus and dorsolateral prefrontal cortex raises the question of their respective roles in the pathophysiology of OCD. The superior temporal gyrus is included in the anterior part of the temporal pole. The temporal pole receives extensive connections from the sensory primary and association cortical areas, and it has dense connections with the affective division of the anterior cingulate cortex, orbitofrontal cortex, amygdala and hypothalamus. 45 Evidence suggests that the ventral portion of the temporal pole is involved in coupling visceral emotional responses with complex visual stimuli, such as those used in the OCD symptom provocation task.46 However, the superior temporal gyrus might be more specifically involved in the pathophysiology of OCD. A morphometric study reported that, compared with individuals without OCD, patients with the disorder had a reduced volume of grey matter in the anterior part of the superior temporal gyrus.47 Maihöfner and colleagues48 found increased spontaneous magnetoencephalographic activity in the left superior temporal gyrus in OCD patients compared with individuals without the disorder. Nevertheless, in both studies, neither the volume of the brain nor the increased magnetoencephalographic activity were correlated with the severity of OCD symptoms, as measured with the Yale–Brown Obsessive Compulsive Scale.47,48 Consequently, these data suggest that the left superior temporal gyrus is involved in the mediation of the anxiety manifestations commonly experienced by patients with OCD rather than in the genesis of obsessive–compulsive symptoms.
The precuneus corresponds to the medial part of the posterior parietal lobule. Its corticocortical connections include other parietal areas, dorsolateral prefrontal cortex, premotor cortex and both the cognitive and affective divisions of the anterior cingulate cortex. The subcortical projections of the precuneus target the dorsolateral caudate nucleus and putamen. 49 Together with the dorsolateral prefrontal and anterior cingulate cortices, this parietal region was found to be involved in self-generated thoughts and in the active reallocation of attentional resources.49–53 It has been reported that this dorsal frontoparietal network may be related to the active inhibition of the attentional processes associated with a cognitive task and to the voluntary shift of attention across sensory modalities.54–57 Thus the likelihood of activation within these cortical areas might be related to patients’ efforts to disregard or to turn their attention away from the obsessive and distressing thoughts induced by the symptom provocation task. This possible interpretation is supported by the negative correlations found between the intensity of OCD symptoms induced during the provocation procedure and the activations found within the dorsal frontoparietal network.10,15
Our results suggest that the cerebral activations observed during the performance of a symptom provocation paradigm were related to several cognitive operations or emotions experienced by patients. First, the cortico–subcortical loops originating in the orbitofrontal cortex and in the cognitive division of the anterior cingulate cortex seem to play a major role in the cognitive processes underlying the emergence of OCD symptoms. Second, the affective division of the anterior cingulate cortex and the left superior temporal gyrus may be more directly involved, through their connections with limbic structures, in the clinical manifestations of anxiety that are usually associated with common symptoms of OCD. Third, the left dorsal frontoparietal network may be involved in patients’ attempts to turn their attention away from their obsessive thoughts.
Limitations
Our findings have to be interpreted in light of several limitations. First, many patients who participated in the selected studies were prescribed medications to treat OCD, which may have influenced the functional activity in the regions of the brain involved in the mediation of OCD symptoms. Of the 8 included studies, 5 involved unmedicated patients, 2 included both medicated and unmedicated patients, 1 included medicated patients only (Table 1). The small number of foci and studies, and the population heterogeneity concerning medication status, did not make it possible to properly assess the potential effect of medication on likelihoods of activation during the performance of the OCD symptom provocation task.
Second, the provocation of symptoms belonging to different symptomatic clusters may have caused differential patterns of functional activation.58–60 The stimuli presented may, by themselves, induce activations through different cerebral networks.60 Unfortunately, the paucity of articles on symptom provocation in patients with OCD did not make it possible to control the wide clinical heterogeneity of the study populations.
Finally, only a very few papers have reported coordinates of activation during obsessive–compulsive symptom provocation in healthy individuals. Thus, to date, no statistical comparison of activation likelihood estimation maps between patients with OCD and healthy individuals can reasonably be performed.
Conclusion
Our study seems to be helpful in highlighting the cortical and subcortical areas involved in performing the OCD symptom provocation task. Our findings confirmed the importance of the cortico–subcortical loops originating in the orbitofrontal and anterior cingulate cortices in the pathogenesis of OCD. They also provide new arguments concerning the putative implication of the temporal cortex in the anxiety manifestations generated by obsessions, especially the hypothetical role of the left dorsal frontoparietal network in resistance to obsessions. To better understand how they interact and lead to the emergence of a given obsessive–compulsive symptom, further research should attempt to determine which regions of the brain are specifically involved in the different cognitive and emotional functions altered in OCD.
Acknowledgements
Dr. Rotge is supported by a grant from the Fondation pour la recherche médicale (Medical Research Foundation). We thank Dr. Ray Cooke for providing advice on English-language wording.
Footnotes
Medical subject headings: obsessive-compulsive disorder; magnetic resonance imaging; positron-emission tomography.
Competing interests: None declared.
Contributors: Dr. Rotge designed the study. Drs. Rotge and Aouizerate acquired the data, which all authors analyzed. Dr. Rotge wrote the article, which Drs. Guehl, Dilharreguy, Cuny, Tignol, Bioulac, Allard, Burbaud and Aouizerate reviewed. All authors gave final approval for publication.
- Received August 7, 2007.
- Revision received November 29, 2007.
- Accepted January 14, 2008.
References

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.