

Abstract
Background: Whether infection with the hepatitis C virus (HCV) causes schizophrenia — and whether the associated risk reverses after anti-HCV therapy — is unknown; we aimed to investigate these topics.
Methods: We conducted a nationwide, population-based cohort study using the Taiwan National Health Insurance Research Database (TNHIRD). A diagnosis of schizophrenia was based on criteria from the International Classification of Diseases, 9th revision (295.xx).
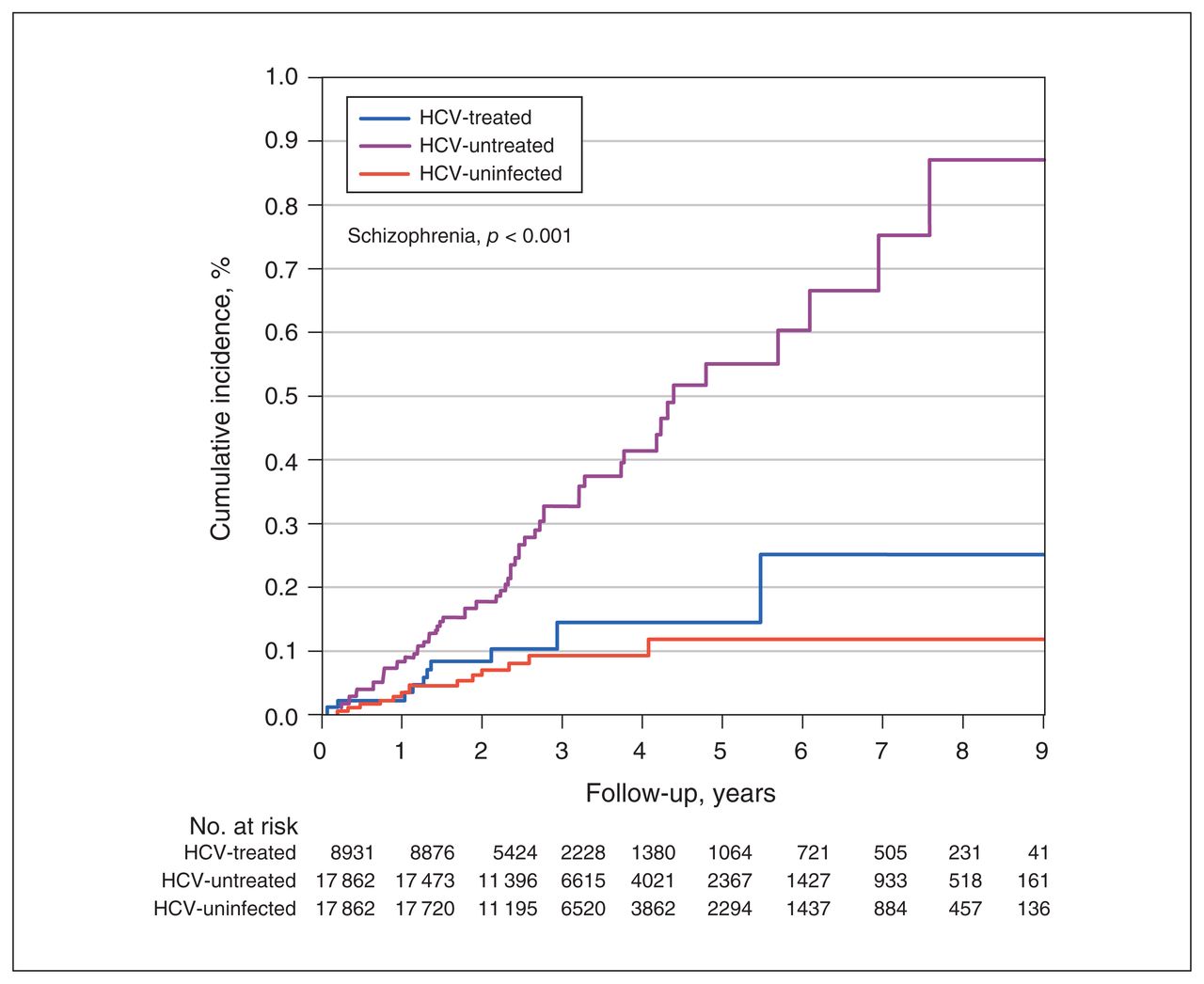
Results: From 2003 to 2012, from a total population of 19 298 735, we enrolled 3 propensity-score-matched cohorts (1:2:2): HCV-treated (8931 HCV-infected patients who had received interferon-based therapy for ≥ 6 months); HCV-untreated (17 862); and HCV-uninfected (17 862) from the TNHIRD. Of the total sample (44 655), 82.81% (36 980) were 40 years of age or older. Of the 3 cohorts, the HCV-untreated group had the highest 9-year cumulative incidence of schizophrenia (0.870%, 95% confidence interval [CI] 0.556%–1.311%; p < 0.001); the HCV-treated (0.251%, 95% CI 0.091%–0.599%) and HCV-uninfected (0.118%, 95% CI 0.062%–0.213%) cohorts showed similar cumulative incidence of schizophrenia (p = 0.33). Multivariate Cox analyses showed that HCV positivity (hazard ratio [HR] 3.469, 95% CI 2.168–5.551) was independently associated with the development of schizophrenia. The HCV-untreated cohort also had the highest cumulative incidence of overall mortality (20.799%, 95% CI 18.739%–22.936%; p < 0.001); the HCV-treated (12.518%, 95% CI 8.707%–17.052%) and HCV uninfected (6.707%, 95% CI 5.533%–8.026%) cohorts showed similar cumulative incidence of mortality (p = 0.12).
Limitations: We were unable to determine the precise mechanism of the increased risk of schizophrenia in patients with HCV infection.
Conclusion: In a population-based cohort (most aged ≥ 40 years), HCV positivity was a potential risk factor for the development of schizophrenia; the HCV-associated risk of schizophrenia might be reversed by interferon-based antiviral therapy.
Introduction
Hepatitis C virus (HCV) is a human pathogen responsible for acute and chronic liver disease that infects an estimated 150 million people worldwide,1 with an estimated global prevalence of 2.8%.2 HCV infection is considered a systemic disease. In addition to causing hepatic complications such as steatosis, cirrhosis and hepatocellular carcinoma, HCV also causes extrahepatic complications, including mixed cryoglobulinemia, renal diseases,3 hypolipidemia, diabetes mellitus, obesity, cardiovascular disease1 and neurologic and psychiatric events.4 Neuropsychiatric disorders have been reported in up to 50% of patients with chronic HCV infection, independent of the severity of the underlying liver disease.4
Schizophrenia is a debilitating psychiatric illness that affects approximately 1.1% of the world’s population, amounting to approximately 51 million people.5 The lifetime prevalence of schizophrenia is approximately 1%, and it commonly follows a chronic course, with onset in late adolescence.6 Schizophrenia contributes to a substantial chronic medical burden and a lifespan that is approximately 15 years shorter than the general population.7 The diverse clinical manifestations of schizophrenia include cognitive, emotional and behavioural abnormalities.6 Current treatments for schizophrenia target mainly psychotic symptoms, do little to ameliorate social or cognitive deficits, and come with adverse effects such as weight gain and diabetes; as well, 30% of people do not respond to them.8
The relationship between schizophrenia and HCV infection has been investigated, but findings have been conflicting. For example, a US study by the Veterans Integrated Services Network showed that patients with schizophrenia had a higher prevalence of HCV infection than the general population (16.5% v. 1.9%).9 Similarly, reported HCV infection rates in patients with schizophrenia are 6.2% in Japan10 and 7.1% and 8.2% in the United States,11,12 higher than the estimated global HCV prevalence (2.8%).2 In contrast, a study showed that the seroprevalence of the HCV antibody was 1.9% in institutionalized patients with chronic schizophrenia,13 and another case–control study showed that the concurrent HCV infection rate was 2.1% in patients with schizophrenia14 — both similar to the prevalence of HCV in the general population. The situation is complicated further when the therapeutic effects of anti-HCV treatment are considered. The combination of pegylated interferon (PEG-IFN) and ribavirin has provided a “cure” for a considerable proportion of patients with chronic HCV infection, particularly patients with the favourable interferon λ 3 (IFNL3) genotype.15 Cure rates have been further improved by replacing interferon-based therapy with potent direct-acting antiviral agents (DAAs).1 The rate of sustained virological response (SVR) to DAAs in HCV-infected patients is approximately 100%.16 Still, although most HCV infections are currently curable with potent DAAs, not all HCV-associated complications are reversed after viral clearance.1,17 Thus, whether HCV infection accelerates the risk of developing schizophrenia and whether the associated risk is reversed after anti-HCV therapy remain crucial issues for public health in an era when HCV infection can be cured using DAAs.
We conducted a nationwide population-based cohort study to investigate the effects of HCV infection on the development of schizophrenia in Taiwan, a country where HCV infection is rampant.18 We investigated the impact of HCV infection on schizophrenia by comparing the cumulative incidence of schizophrenia and of overall mortality among HCV-infected people with and without anti-HCV therapy, and among people without HCV infection.
Methods
Samples and measurements
This population-based retrospective cohort study used national-level data from the Taiwan National Health Insurance Research Database (TNHIRD), including the National Health Insurance (NHI) administrative database, the cancer registry database and the death registry database. The mandatory, single-payer NHI program provides comprehensive coverage of ambulatory care, laboratory tests, hospital services and prescription drugs. More than 99% of the population is enrolled in the program, and approximately 92% of health care organizations are contracted with the NHI administration. We did not enrol patients who had schizophrenia before they started anti-HCV treatment in the HCV-treated cohort, or before baseline in the other cohorts. Because Taiwan is a hyperendemic area for hepatitis B virus infection, which profoundly affects HCV viral load and biases the phenotype of HCV infection,19 we excluded patients who were infected with hepatitis B virus during the observation period (2003–2012). We also excluded patients with cirrhosis-related complications such as hepatoencephalopathy, esophageal varices, ascites or hepatorenal syndrome to avoid interference from complications or from associated treatments. In particular, given that some infections such as toxoplasmosis,20,21 Chlamydophila pneumoniae,22 lymphocytic choriomeningitis virus23 and herpes simplex virus type 124 have been reported to affect the development of schizophrenia, we excluded patients with these infections.
The HCV-treated cohort included patients who had an HCV RNA test and received ribavirin and PEG-IFN between 2003 and 2012. The date of their first HCV test was assumed to be the index date of their diagnosis. Baseline for the HCV-treated cohort was 6 months after they had completed combination therapy, which is the time to ensure SVR. Only those who had undergone anti-HCV therapy for 6 months or more were enrolled. The HCV-untreated cohort included patients who had an HCV test (HCV antibody or HCV RNA test; their first HCV test was the index date); were diagnosed with hepatitis C (International Classification of Diseases, 9th revision, clinical modification [ICD-9-CM] codes 070.41, 070.44, 070.51, 070.54, 070.70, 070.71 or V02.62); were prescribed a hepatoprotective agent (silymarin, liver hydrolysate, choline bitartrate or ursodeoxycholic acid); and did not receive any anti-HCV therapy (ribavirin or PEG-IFN). The HCV-uninfected cohort included those who had no diagnosis of HCV and no HCV test, and who received no hepatoprotective agents or anti-HCV therapy. Only those without schizophrenia-related NHI claims at least 2 years before baseline were included in the 3 cohorts.
We matched the HCV-treated cohort with the HCV-untreated and HCV-uninfected cohorts (1:2:2) using a propensity score–matching method that indicated the probability of receiving combination therapy and was estimated using a logistic model. Covariates in the model included age group (20–39, 40–49, 50–59, ≥ 60 years), sex (male, female), NHI registration location (urban, township, rural), Charlson Comorbidity Index score (0, 1, ≥ 2)25 and the year of the index date (2003–2006, 2007–2009, 2010–2012). We used this method to ensure that the HCV-treated cohort and their selected counterparts were comparable in terms of observed characteristics. We assigned the baseline for the HCV-untreated and HCV-uninfected cohorts according to the period from the index date to baseline (6 months after treatment completion) for their matched counterparts. The index date for those in the HCV-uninfected cohort was the date of a physician visit randomly selected from their claims database. The matching process for the 3 cohorts is shown in Appendix 1, Figure S1, available at jpn.ca. Outcomes were the development of schizophrenia or mortality. Schizophrenia was defined as follows: at least 1 hospitalization with a schizophrenia diagnosis (ICD-9-CM code 295.xx); at least 2 outpatient visits with a schizophrenia diagnosis; or at least 1 outpatient visit with a schizophrenia diagnosis and at least 1 antipsychotic prescription within 1 year. Patients were followed until the date of an event (schizophrenia), death or the end of follow-up (December 31, 2012), whichever came first. For the HCV-treated group, we recorded only schizophrenia diagnoses or death that occurred more than 6 months after the completion of anti-HCV therapy. Dates of death were taken from the death registry database.
Statistical analysis
We performed all statistical analyses using SAS statistical software (version 9.4; SAS Institute Inc.). We estimated cumulative incidences of outcomes and compared them using the modified Kaplan–Meier method and the Gray method; death was a competing risk event.26 We used Cox proportional hazards models, taking competing mortality into account, to estimate adjusted hazard ratios for developing schizophrenia — adjusting for age; sex; the interaction of age and sex; NHI registration location; Charlson Comorbidity Index score; year of index date; and the baseline presence of liver cirrhosis, chronic obstructive pulmonary disease, end-stage renal disease, diabetes mellitus, hypertension, dyslipidemia, cardiovascular events (including percutaneous coronary intervention, coronary artery bypass graft, myocardial infarction, heart failure, cardiogenic shock and peripheral vascular disease) and stroke. We checked and confirmed proportionality assumptions using time-dependent explanatory variables. We checked for multicollinearity and excluded variables that were highly correlated with other variables. We conducted a post hoc power analysis to assess the powers of the tests used in this study. Statistical significance was set at 5% based on 2-tailed tests of the null hypothesis.
Institutional review board
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the local institutional review board.
Results
Baseline characteristics
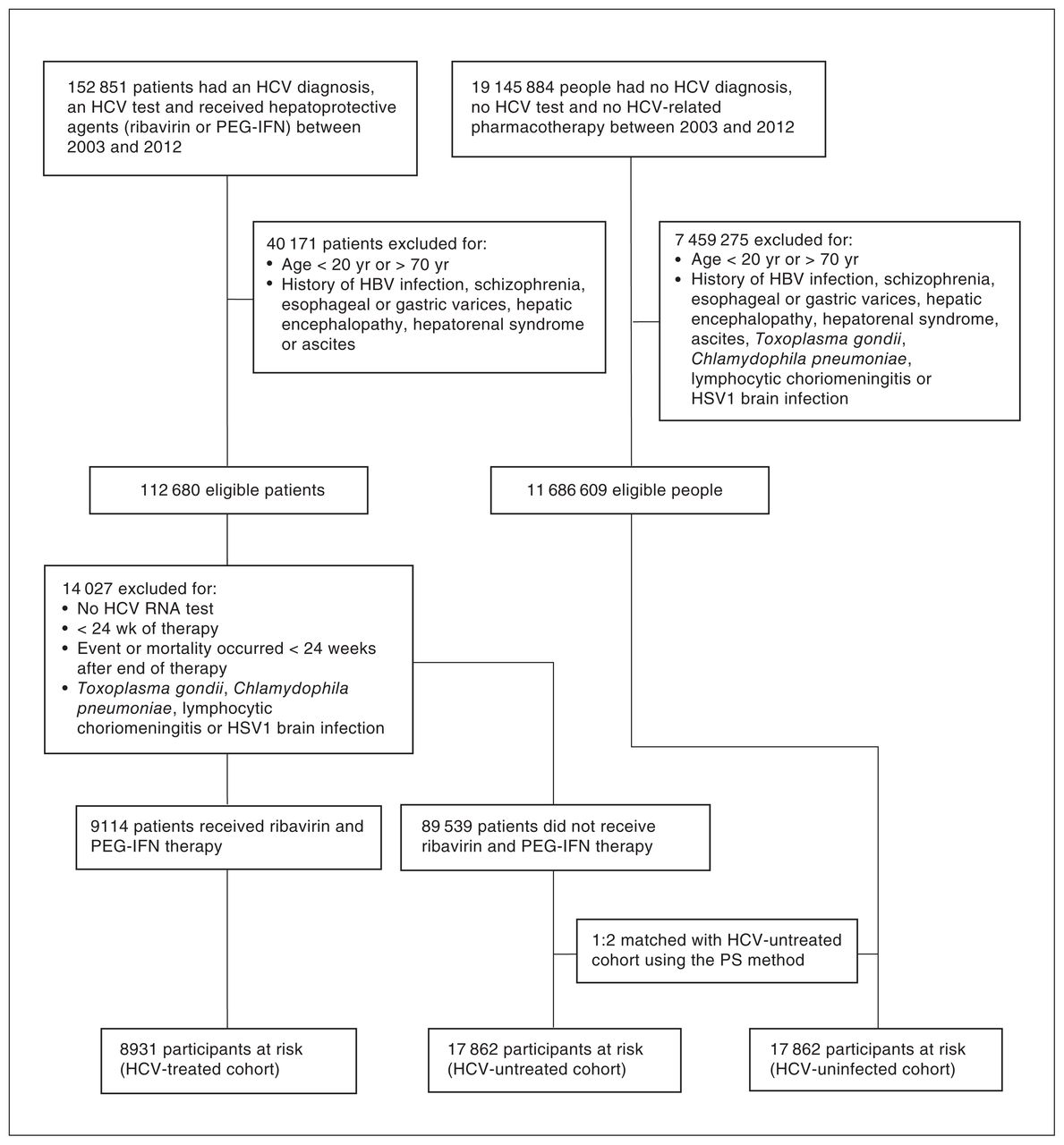
From a total of 19 298 735 patients registered in the TNHIRD database between January 1, 2003, and December 31, 2012, 112 680 patients with HCV infection and 11 686 609 patients without HCV infection were eligible for the study. We enrolled patients in 1 of 3 cohorts: HCV-treated (n = 8931), HCV-untreated (n = 17 862) and HCV-uninfected (n = 17 862; Figure 1). The 3 cohorts were matched using propensity scores and did not differ in terms of demographic factors, NHI registration location, Charlson Comorbidity Index score or index year — the covariates used to calculate propensity scores in the models; baseline comorbidities differed. Of the total sample (n = 44 655), 82.81% (n = 36 980) were age 40 years or older (Table 1). Compared to the HCV-untreated cohort, the HCV-treated cohort had higher rates of baseline cirrhosis but lower rates of end-stage renal disease, diabetes mellitus, hypertension, dyslipidemia, cardiovascular events and stroke. Compared to the HCV-uninfected cohort, the HCV-treated cohort had higher rates of baseline cirrhosis, chronic obstructive pulmonary disease and end-stage renal disease, but lower rates of dyslipidemia and stroke. Compared to the HCV-uninfected cohort, the HCV-untreated cohort had higher rates of all baseline comorbidities except stroke. To delineate which complications were associated with HCV infection, we compared baseline factors between an HCV-infected cohort (a combination of the HCV-treated and HCV-untreated cohorts) and the HCV-uninfected cohort. The HCV-infected cohort had higher rates of all baseline comorbidities, except for dyslipidemia and stroke (Appendix 1, Table S1).

Flow chart of Taiwan National Health Insurance Research Database study sample selection. HBV = hepatitis B virus; HCV = hepatitis C virus; HSV = herpes simplex virus; PEG-IFN: pegylated interferon; PS = propensity score.
Participant baseline characteristics
Cumulative incidence of schizophrenia and associated risk factors
We followed the 3 cohorts (HCV-treated, HCV-untreated and HCV-uninfected until death, for a duration of up to 9.5 years). The results of the post hoc power analysis for the various comparisons were greater than 0.8 (Appendix 1, Table S2). Of the 3 cohorts, the HCV-untreated cohort had the highest cumulative incidence of schizophrenia (Figure 2, Table 2). However, we observed no difference in cumulative incidence of schizophrenia between the HCV-treated and HCV-uninfected cohorts. Multivariate analysis of the 3 cohorts showed that the HCV-untreated cohort had a higher risk of developing schizophrenia than the HCV-treated and HCV-uninfected cohorts, and that patients with baseline stroke had borderline higher risk than those without baseline stroke (Appendix 1, Figure S2).

Cumulative incidence of schizophrenia among the 3 Taiwan National Health Insurance Research Database cohorts: HCV-treated, HCV-untreated and HCV-uninfected. HCV = hepatitis C virus.
Comparison of the cumulative incidence of schizophrenia among the study cohorts
Because the HCV-treated and HCV-uninfected cohorts showed similar risks of developing schizophrenia, we combined these cohorts into an HCV-negative cohort to explore the effect of HCV on the development of schizophrenia. Compared to the HCV-negative cohort, the HCV-positive (i.e., HCV-untreated) cohort had a higher risk of incident schizophrenia (p < 0.001; Appendix 1, Table S3). Multivariate analyses of these 2 cohorts showed that HCV positivity (hazard ratio 3.469, 95% confidence interval [CI] 2.168–5.551) was an independent risk factor for the development of schizophrenia (Figure 3).

Forest plot of factors associated with incident schizophrenia in the 2 Taiwan National Health Insurance Research Database cohorts: HCV-positive (HCV-untreated) and HCV-negative (combination of HCV-treated and HCV-uninfected). CCI = Charlson Comorbidity Index score; HCL = higher confidence interval limit; HCV = hepatitis C virus; HR = hazard ratio; LCL = lower confidence interval limit.
Cumulative incidence of mortality
Of the 3 cohorts, the HCV-untreated cohort had the highest cumulative incidence of overall mortality at 9.5 years (20.799%, 95% CI 18.739%–22.936%; p < 0.001); the HCV-treated (12.518%, 95% CI 8.707%–17.052%) and HCV-uninfected cohorts (6.707%, 95% CI 5.533%–8.026%) had similar mortality rates (p = 0.12; Appendix 1, Table S4).
Discussion
The differences in baseline comorbidities between the HCV-treated and HCV-untreated cohorts coincided with the fact that only patients with significant hepatic fibrosis were reimbursed for anti-HCV therapy, and those with severe comorbidities were ineligible for interferon-based therapy. The differences in comorbidities between the HCV-infected and HCV-uninfected cohorts reflected the fact that HCV is associated with cardiometabolic complications and that people infected with HCV are less likely to have dyslipidemia.1 Thus, our baseline comparisons of the 3 cohorts supported the reliability of the results from the TNHIRD.
Although high HCV infection rates have been noted in patients with schizophrenia, the data are conflicting,9–14 and high comorbidity with intravenous substance use11 or old age10 in patients with schizophrenia has been thought to account for the high HCV prevalence in this population. The present study clearly demonstrated that HCV infection increased the risk of incident schizophrenia: the HCV-untreated cohort had the highest cumulative incidence of schizophrenia of the 3 cohorts, and multivariate analyses showed that HCV infection was positively associated with the development of schizophrenia. Previous findings that patients with schizophrenia had a higher prevalence of chronic liver disease than the general population, and comorbidity with diabetes was the primary risk factor for patients with schizophrenia to develop chronic liver disease,9,27 endorse a causal relationship between HCV infection and schizophrenia, because HCV infection is a main cause of both chronic liver disease and diabetes.1 Although schizophrenia is a psychiatric disorder with high heritability, the etiology of schizophrenia is complex and involves a complicated interplay of genetic and environmental factors.28 Infection, obstetric complications, urbanicity, cannabis and trauma have all been shown to interact with genetic risk.29 With respect to infection, associations between schizophrenia and toxoplasmosis, herpes or influenza have been reported,20–24,28 and we eliminated patients with these infections to avoid any confounding effects. Interestingly, 8% of the human genome consists of human endogenous retroviruses (HERVs) and a specific HERV — HERV-W — has been linked with schizophrenia.28 A lifelong scenario of a detrimental interaction between infectious agents and HERV-W genes may cause the development of schizophrenia.29 The evidence of direct neuroinvasion of HCV, particularly in cells of the macrophage or monocyte lineage,30 suggest the possibility that HCV interacts with HERV-W in initiating the development of schizophrenia. As well, inflammation, oxidative stress31 and disturbances in neurotransmitter, metabolism, immunity and adipokine homeostasis32 may play important roles in eliciting schizophrenia. HCV infection consistently causes significant alterations in metabolism,1,33,34 neurotransmitter,34 immunity, adipokine15 and oxidative stress profiles1,33,34 in the hosts, reflecting the potential link between HCV and schizophrenia. It is important to note that the typical age of onset for schizophrenia is late adolescence or the early 20s,6 whereas most of the patients in our study (82.81%) were aged 40 years or older. That is, most of the diagnoses of schizophrenia in the present study occurred after age 40 years, because only those with no schizophrenia-related claims at least 2 years before baseline were enrolled. This finding was in line with the fact that the HCV infection rate is highest for adults older than 35 years,35 because the present study was based on propensity score–matched HCV-positive and HCV-negative cohorts. The late onset of schizophrenia in these patients thus might not be generalizable for patients with schizophrenia and requires further investigation.
Although interferon-based anti-HCV therapy in patients with schizophrenia has yielded negligible worsening psychiatric symptoms and the therapeutic response rate for people with schizophrenia is similar to that of the general population,36 schizophrenia is still a predictive factor for not treating HCV infection because of concerns about interferon-related neuropsychiatric adverse effects.37 We stress that the HCV-associated risk in incident schizophrenia might be reversed by interferon-based anti-HCV therapy, because the cumulative incidence of schizophrenia in the HCV-treated cohort was lower than that of the HCV-untreated cohort and similar to that of the HCV-uninfected cohort. However, whether the reversal of HCV-associated risk in schizophrenia is universal for all anti-HCV regimens (including DAAs) or is specific to interferon-based therapy requires further investigation. Moreover, the HCV-untreated cohort in the present study had the highest risk of overall mortality among the 3 cohorts. It is likely that this finding was at least partly attributable to HCV-associated systemic complications.1–4 As well, people with schizophrenia are at greater risk for morbidity and mortality as a result of cardiovascular disease38 and stroke39 than the general population. Thus, mortality is high for those with schizophrenia and HCV infection.40 These findings point to the importance of prescribing anti-HCV therapy in all HCV-infected patients regardless of schizophrenia status (unless contraindicated), particularly in the era of DAAs, which can cure HCV infection. In addition to HCV infection, stroke was borderline positively associated with the development of incident schizophrenia. Schizophrenia-like psychosis after stroke is common and severely affects quality of life.41 Preexisting subcortical atrophy and a lesion location in the right hemisphere42 — particularly in the frontal, temporal and parietal regions and the right caudate nucleus41 — are risk factors for post-stroke schizophrenia-like psychosis.
Limitations
The current study had several limitations. First, because the TNHIRD did not contain direct laboratory results, it was impossible to explore a correlation between schizophrenia and SVR to anti-HCV therapy. However, we were confident of antiviral efficacy in the HCV-treated cohort because interferon-based therapy generally achieves a high SVR in Taiwan (up to 82.7%),15 where a favourable IFNL3 genetic variation for interferon-based therapy response is prevalent.15 Second, there might have been some patients with undiagnosed HCV infection in the HCV-uninfected cohort. However, given that reimbursement for anti-HCV therapy is nationwide and only 2.7% of the Taiwanese were likely to be infected with HCV,43 the rate of undiagnosed HCV infection in the HCV-uninfected cohort was probably negligible and likely would not bias our results. Third, information about important risk factors for schizophrenia, including genetic susceptibility, were lacking in the TNHIRD and the effect of these risk factors on schizophrenia could not be assessed. Fourth, we were unable to determine the precise mechanism of the increased risk of schizophrenia in patients with HCV infection. Future prospective studies in other independent cohorts with identifiable SVR following DAA-based anti-HCV therapy, comprehensive surveys of risk factors, well-stratified patient subpopulations and sophisticated molecular or animal investigations are needed to elucidate the fundamental mechanisms that underlie the findings described here.
Conclusion
Taken together, the findings of the present study confirmed that in a population aged mostly 40 years and older, HCV positivity is a positive risk factor for incident schizophrenia, and that the risk may be reversed with interferon-based antiviral therapy. In the era of DAAs to eliminate HCV infection, anti-HCV therapy should be prescribed for all people infected with HCV to reduce the risk not only of hepatic complications, but also of extrahepatic complications, including schizophrenia.
Acknowledgments
The authors thank Ms. Shu-Chun Chen from the Liver Research Center, Chang Gung Memorial Hospital, Taiwan, for assistance with data mining.
Footnotes
Funding: This study was supported by grants from the Chang Gung Medical Research Program (CMRPG3I0412, CMRPG3K0721 and CMRPG1K0111) and the National Science Council (MOST 110-2314-B-182-044-, MOST 109-2314-B-182-024- and MOST 109-2629-B-182-002-). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The opinions expressed in this paper are those of the authors and do not necessarily represent those of Chang Gung Medical Hospital and National Science Council, Taiwan.
Competing interests: None declared.
Contributors: M. Lin and M.-L. Chang designed the study. J. Hu and R. Chien acquired the data, which J. Cheng, M.-Y. Chang and H. Ku analyzed. All authors wrote the article. All authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
- Received November 1, 2020.
- Revision received July 7, 2021.
- Accepted July 26, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.