

Abstract
Background: The possibility of using noninvasive brain stimulation to treat mental disorders has received considerable attention recently. Repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) are considered to be effective treatments for depressive symptoms. However, no treatment recommendation is currently available for anxiety disorders, suggesting that evidence is still limited. We conducted a systematic review of the literature and a quantitative analysis of the effectiveness of rTMS and tDCS in the treatment of anxiety disorders.
Methods: Following PRISMA guidelines, we screened 3 electronic databases up to the end of February 2020 for English-language, peer-reviewed articles that included the following: a clinical sample of patients with an anxiety disorder, the use of a noninvasive brain stimulation technique, the inclusion of a control condition, and pre/post scores on a validated questionnaire that measured symptoms of anxiety.
Results: Eleven papers met the inclusion criteria, comprising 154 participants assigned to a stimulation condition and 164 to a sham or control group. We calculated Hedge’s g for scores on disorder-specific and general anxiety questionnaires before and after treatment to determine effect size, and we conducted 2 independent random-effects meta-analyses. Considering the well-known comorbidity between anxiety and depression, we ran a third meta-analysis analyzing outcomes for depression scores. Results showed a significant effect of noninvasive brain stimulation in reducing scores on disorder-specific and general anxiety questionnaires, as well as depressive symptoms, in the real stimulation compared to the control condition.
Limitations: Few studies met the inclusion criteria; more evidence is needed to strengthen conclusions about the effectiveness of noninvasive brain stimulation in the treatment of anxiety disorders.
Conclusion: Our findings showed that noninvasive brain stimulation reduced anxiety and depression scores compared to control conditions, suggesting that it can alleviate clinical symptoms in patients with anxiety disorders.
Introduction
Anxiety disorders are the most prevalent class of mental disorder in most Western societies1,2 and are one of the foremost causes of disability.3 (For epidemiologic details, see Craske and colleagues.4) The onset of anxiety disorders typically occurs in young adulthood.5 Then, they seem to take a chronic course, characterized by remitted and relapsed periods; the stability of the disease across time varies among studies and specific diagnoses.4,6
According to DSM-5,7 anxiety disorders include specific phobias, social anxiety disorder, panic disorder, agoraphobia and generalized anxiety disorder (posttraumatic stress disorder and obsessive–compulsive disorders no longer fall in this grouping, and have not been considered in this meta-analysis). The DSM-5 diagnostic criteria for anxiety are similar to those of the other standard classification system, the International Classification of Diseases, tenth edition (ICD-10).8 In both systems, anxiety disorders are a spectrum of multidimensional phenotypes9 that share clinical features, such as excessive and stable anxiety; physiologic symptoms, such as tachycardia and chest tightness; and typical behavioural responses, such as avoiding perceived threats, places or situations, that impair people’s psychological well-being and quality of life.
The neurobiology of anxiety disorders is still unclear. Studies have been conducted with small participant samples, and with heterogeneous imaging methods, paradigms and patient comorbidities.10 Although disease-specific differences exist, converging evidence suggests that in general, anxiety disorders are characterized by structural and functional alterations that primarily involve a mesocorticolimbic pathway (see Duval and colleagues11 for a review). According to this neurobiological account, the amygdala, the prefrontal cortex, the anterior cingulate cortex, the hippocampus and their functional connections might play a key role in generating and regulating fear, anxiety and threat detection.4,9 Hyperactivity in the amygdala is one of the most consistent findings.12,13 Such abnormal activity has been reported across several specific diseases and tasks, such as anxiety-provoking public speaking,14–16 fear-conditioning17,18 or presentation tasks that involve emotional images or threatening faces in social phobia or social anxiety disorder.19,20 Moreover, activation of the amygdala has been positively correlated with symptom severity21,22 and decreases after intervention with medication and psychotherapy.22–25 The response of the amygdala to threat is regulated via bidirectional connections to the anterior cingulate cortex and ventromedial prefrontal cortex in animals and humans.26,27 In line with this finding, human neuroimaging studies have highlighted hypoactivity in the prefrontal cortex in anxious patients, suggesting that amygdala hyperactivity might be the result of a decrease in top–down inhibitory control exerted by the prefrontal cortex28–31 (but see Kraus and colleagues32 for different results). Considering the functional abnormalities seen in anxiety disorders, it has been suggested that an interhemispheric imbalance might be at their basis, involving hypoactivation of the left dorsolateral prefrontal cortex (dlPFC) and hyperactivation of the right dlPFC.33–35
First-line treatments for anxiety comprise pharmacological or psychotherapeutic interventions; cognitive-behavioural therapy is considered the most effective treatment, according to several international guidelines.36,37 However, a consistent number of patients fail to respond to traditional treatment or experience relapse and recurrence of their symptoms.38,39 In the search for alternative treatments over the last 30 years, interest in the use of noninvasive brain stimulation has grown rapidly, as a standalone therapy or combined with cognitive or behavioural interventions.40–42 The rationale for using noninvasive brain stimulation in psychiatric treatment is the possibility of rebalancing maladaptive activity and functional connectivity between brain structures. Indeed, there is a consensus that in addition to genetic, hormonal, social and cognitive factors, psychiatric disorders also involve pathologically altered neural plasticity, which can be modulated through noninvasive brain stimulation, with biochemical effects that outlast the time of stimulation.43 (For recent reviews, see Kronberg and colleagues44 and Ziemann.45) Although the precise mechanisms of action are still under investigation, the effects of noninvasive brain stimulation on synaptic plasticity involve several phenomena, ultimately leading to long-term potentiation (synaptic strengthening) and long-term depression (or synaptic weakening) processes.46 (For a review and discussion, see Cirillo and colleagues.47)
Among noninvasive brain stimulation techniques, the 2 most commonly used are transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). TMS is a technique based on delivering a strong, short magnetic pulse to the patient’s head, inducing neuronal firing by suprathreshold neuronal membrane depolarization.48 When used to generate long-term effects, TMS is typically applied using repetitive (rTMS) protocols, with inhibitory (≤ 1 Hz and continuous theta-burst stimulation) or excitatory (> 5 Hz and intermittent theta-burst stimulation [iTBS]) protocols.49 tDCS is a neuromodulatory technique in which weak constant direct current (typically 1–2 mA) is delivered through the scalp using 2 electrodes, 1 with a positive (anode) polarity and 1 with a negative (cathode) polarity.50 tDCS does not generate action potentials per se, but it does induce small changes at the membrane potential level, influencing spike frequency and, in turn, cortical excitability.51,52 The effects of tDCS are polarity-dependent: anodal stimulation depolarizes the neuronal membrane and cathodal stimulation hyperpolarizes it, increasing and decreasing cortical excitability, respectively.53
Of the parameters for noninvasive brain stimulation, stimulation frequency for TMS (high or low) and polarity for tDCS (either anodal or cathodal) are usually considered the determinants of an expected effect in cortical excitability and behaviour: excitatory-enhancing or inhibitory-disrupting. Although a detailed discussion of the 2 techniques goes beyond the scope of this meta-analysis, it is crucial to point out that such an expectation can be misleading. Indeed, the outcomes of noninvasive brain stimulation — in terms of both cortical excitability and behavioural modulation — cannot be clearly determined in advance. They are the result of more complex interactions involving stimulation parameters (intensity, orientation), cerebral regions and their connections, individual anatomic features, and state dependency.54–57
Among psychiatric disorders, the main field in which noninvasive brain stimulation is applied as an alternative treatment is major depressive disorder (MDD). The clinical use of rTMS to treat MDD was approved by the US Food and Drug Administration in 2008 using high-frequency (10 Hz) left-side stimulation of the dlPFC and in 2018 using iTBS over the same region.58 The effectiveness of rTMS and tDCS for other psychiatric disorders has been explored in several reviews and meta-analyses targeting schizophrenia,59,60 substance abuse61 and obsessive–compulsive disorder62,63 with promising but preliminary results.
To provide shared recommendations for good practice, periodically updated guidelines from independent expert panels have reviewed and analyzed studies investigating rTMS64,65 and tDCS66,67 protocols for a broad spectrum of neurologic and psychiatric disorders. According to the guidelines’ levels of classification, level A (“definitely effective or ineffective”) indicates that the evidence was sufficient (in terms of number and quality of studies) to establish whether or not a specific protocol applied over a certain region was useful for a particular disorder. Only a few protocols have reached level A. For TMS, the protocols with level A effectiveness are as follows: high-frequency rTMS applied to the left dlPFC to treat depression, high-frequency TMS to the primary motor cortex contralateral to the painful side for neuropathic pain, and low-frequency rTMS applied over the contralesional primary motor cortex for hand motor recovery in the post-acute stage of stroke.65 For tDCS, level A effectiveness has been assigned only to anodal stimulation over the left dlPFC in depression;66 anodal tDCS over the ipsilesional primary motor cortex is considered definitely not effective for enhancing robotic therapy in motor rehabilitation for subacute stroke. To date, no recommendation has been made for the use of rTMS or tDCS in the treatment of anxiety disorders; the available data are not sufficient to make recommendations, either for its use or to claim an absence of effect.65,66
To fill this gap in the literature, several recent reviews have examined the available literature related to the therapeutic effects of rTMS and tDCS in the treatment of anxiety disorders,35,68 anxiety symptoms arising from other pathologies69 and specific anxiety disorders (e.g., generalized anxiety disorder70). These reviews testify to the general interest in this topic and have shown promising yet preliminary results. However, so far they have included single-case studies and protocols without a control condition, providing an overview of the state of the art, but without cumulatively quantifying the results. To our knowledge, 3 meta-analyses71–73 have investigated the efficacy of rTMS from a quantitative perspective. Cui and colleagues72 investigated the efficacy of rTMS in treating generalized anxiety disorder. They included 21 studies (2 in English and 19 in Chinese), all with a control group receiving sham rTMS or no intervention, suggesting that rTMS was a useful option for decreasing the symptoms of generalized anxiety disorder. Trevizol and colleagues73 investigated the efficacy of rTMS in randomized clinical trials of anxiety disorders. Their review included 14 papers, but 5 of those investigated posttraumatic stress disorder and 8 investigated obsessive–compulsive disorder, both of which are now considered independent diagnostic categories.7 The authors concluded that TMS was not superior to the sham condition in reducing anxiety symptoms. In line with this, Cirillo and colleagues71 conducted a systematic review and analysis in anxiety and posttraumatic stress disorder that included 17 papers: 9 considering posttraumatic stress disorder, 2 specific phobias, 2 panic disorder, and 4 generalized anxiety disorder. The authors ran 2 independent meta-analyses: 1 for posttraumatic stress disorder and 1 for generalized anxiety disorder. They considered the mean difference in pre- and post-treatment scores for sham stimulation versus TMS when the 2 conditions were available, and for the mean difference in pre/post scores for TMS when sham stimulation was not tested. The results showed substantial treatment efficacy for both disorders.
To our knowledge, no previous meta-analyses have combined TMS and tDCS to investigate the effectiveness of noninvasive brain stimulation in treating anxiety disorders. Moreover, some of the previous reports included research that did not involve a control group or involved disorders that are now considered to be separate nosological entities. In the present study, we aimed to qualitatively assess and quantitatively evaluate the effect of rTMS and tDCS protocols in anxiety disorders. We also aimed to overcome the limitations of individual studies, which have been typically conducted using small sample sizes and applying heterogeneous stimulation parameters and different numbers of sessions.35
Similar to anxiety, a neurobiological pattern of imbalance of cortical excitability between the right and left dlPFC has been reported in MDD,74–76 in line with the frequent comorbidity of the 2 disorders.77–79 Indeed, although anxiety and depression have been considered to be nosologically independent categories according to traditional classifications, their comorbidity is common, with reported overlap rates of 40%–50% (see Choi and colleagues80 and Ionescu and colleagues81 for reviews). However, despite this clinical evidence, the comorbidity between anxiety and depression is often overlooked in the literature, possibly because of a lack of a clear and noncontroversial definition (see Ionescu and colleagues81). We reasoned that the stimulation of brain areas involved in anxiety and mood disorders might also produce changes in depressive symptom scores; for this reason, we included studies in which patients had an additional depression diagnosis in our meta-analysis and when pre/post scores from depressive symptoms questionnaires were available, we analyzed those as well.
Methods
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines82,83 to conduct this systematic review and meta-analysis (Appendix 1, available at jpn.ca).
Literature search
We used PubMed, Web of Science and Scopus to select peer-reviewed original papers published in English before the end of February 2020, exploring the application of rTMS or tDCS in patients with anxiety disorders. We combined key words for brain stimulation techniques (“rTMS,” “tDCS”) with relevant anxiety disorder labels (“generalized anxiety disorder,” “agoraphobia,” “panic disorder,” “specific phobia,” “social anxiety”). We excluded non-English papers, case reports, systematic and narrative reviews, meta-analyses, conference proceedings and abstracts. We also excluded reports that measured anxiety in nonclinical populations, reports without a sham or behavioural control condition, and reports without at least 1 validated clinical questionnaire. When multiple papers were based on the same data set, we included only the oldest paper reporting the results relevant to our meta-analysis — namely the effect of stimulation treatment on anxiety and depressive symptom questionnaire scores.
Records screening and data extraction
To blind the screening process, we used Rayyan (rayyan.qcri.org/), a web and mobile systematic reviews manager.84 After duplicates had been removed, 3 researchers (A.V., A.G., A.P.) independently categorized the records as “include,” “exclude” or “maybe” based on titles and abstracts. Reasons for exclusion were specified by defined labels based on the inclusion and exclusion criteria. Then, the same 3 researchers analyzed the full texts of the remaining records and independently selected eligible studies. When the full versions of articles were not available, we contacted the corresponding authors. In both the title–abstract and full-text screening phases, conflicting decisions were solved by consensus. One researcher (A.P.) extracted data using a structured form, and the data were checked for consistency and accuracy by the other 2 authors (A.V., A.G.). Discrepancies were resolved by consensus.
We extracted anxiety and depression questionnaire scores for the treatment and control groups from the included studies. Because at least 2 measures of anxiety were available for each study, we decided to code them in 2 separate meta-analyses. The first meta-analysis targeted questionnaire scores that investigated symptoms specific to the disorder for which participants were included in the study (e.g., for panic disorder, “Please indicate how many panic and limited symptoms attacks did you have during the week?”). The second meta-analysis considered a more general core typically related to all anxiety symptoms (e.g., “Please indicate how much you were bothered by feeling unable to relax in the last month.”). When measures of depressive symptoms were available, we also collected these.
Study quality assessment
Two researchers (A.V., A.G.) independently assessed the quality of the studies based on the criteria in the Cochrane Collaboration’s risk-of-bias tool:85 random sequence generation, allocation concealment, blinding strategy, incomplete outcome data and selective outcome reporting. To determine selection bias, we rated random sequence generation as low-risk only when randomization procedures were reported (e.g., random number table, computer-generated randomization, randomization envelopes). We rated allocation concealment as low-risk only for studies that recruited a group of patients who received sham stimulation. To determine reporting bias, we checked the registered protocol of the included records when available. Conflicts were solved by consensus of the 2 researchers and by consulting a third researcher when needed (A.P.).
Quantitative analysis
For each included study, we extracted relevant information, including means and standard deviations of scores on clinical scales, the noninvasive brain stimulation protocol (technique, number of sessions, stimulation location), and patient characteristics. As the primary outcome measure, we extracted the pre/post-treatment mean difference in anxiety-disorder-specific scales (10 studies included) for the treatment and control groups to measure the effect of the noninvasive brain stimulation protocol on anxiety symptoms. When information in the text, tables or supplementary material was insufficient, we contacted the authors to obtain missing data.86–88 We calculated the standard deviation (SD) of the change score (pre- to post-noninvasive brain stimulation treatment), as suggested by the Cochrane Handbook for Systematic Reviews of Interventions:89

where corr was the correlation between pre- and post-measurement variances, set at 0.5 as suggested by Follman and colleagues.90
We computed sampling variance, standardized mean difference (SMD) and summary analyses for each included study, using the “escalc” function of the “metafor” package in R (version 3.4.3).91,92 We corrected SMD for positive bias for a small group within the function, calculating Hedge’s g,93 which we used as a measure of effect size. We calculated the global effect of noninvasive brain stimulation in reducing anxiety symptoms using a random-effects model with the “rma” function of the “metafor” package in R. Random-effects meta-analyses can account for heterogeneity due to sampling errors and large variations in effect size.94 Studies vary in their characteristics (e.g., patient characteristics, stimulation interventions, associated therapies), and this influences the effect size. Therefore, the included studies represent only a portion of the possible population of studies to be performed. This motivated our decision to include random effects in our analyses. We also assessed heterogeneity through variation because of sampling errors (Q statistic) and the percentage of variation between studies because of heterogeneity rather than chance (I2 statistics).95 We identified potential outliers with an analysis of influence,96–98 implemented using the “inf” function of the “metafor” package in R. We controlled for publication bias using funnel plots, Egger’s regression test99 and the rank correlation test,100 and eventually corrected any bias using the “trim and fill” method,101 which creates dummy potential missing studies to create a more symmetric funnel plot.
Finally, we ran an exploratory moderation analysis. In noninvasive brain stimulation, some features are crucial for the final outcome, such as the number of sessions, the type of stimulation, the interaction between brain areas and the type of stimulation. However, given the limited number of studies in the meta-analysis, we could not include all of the potentially interesting moderators. Therefore, we included only the informative ones — namely those that were sufficiently represented in the selected papers. We adopted the same procedures for the secondary outcome measures: general anxiety scale ( Hamilton Anxiety Rating Scale [HAM-A] or Beck Anxiety Inventory [BAI]; 9 studies included) and depressive interview/self-report questionnaire (Hamilton Depression Rating Scale [HAM-D] or Beck Depression Inventory; 7 studies).
Results
Study selection
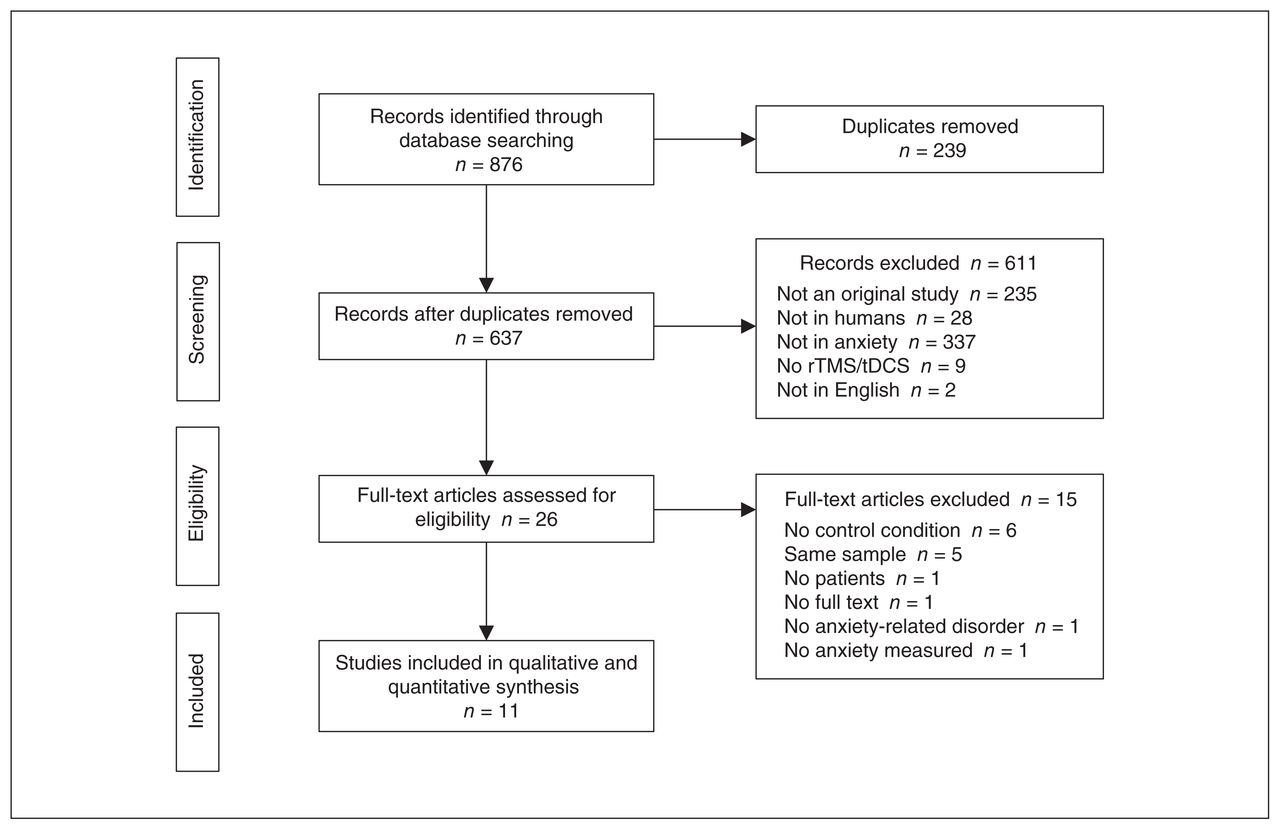
We identified a total of 876 publications. We removed 239 duplicates and carefully reviewed the titles and abstracts of the remaining 637 records. Of these, we excluded 611 records because they did not meet our inclusion criteria. We then examined the full texts of the remaining 26 papers and excluded 15 records at this stage. We excluded 6 studies because they did include a control condition (sham stimulation or a control group).102–107 We excluded 5 studies because they involved samples already analyzed in previous articles. (When multiple reports were published on the same study sample, we included reports according to publication date; the oldest paper was always included in our analyses. We also checked that subsequent reports did not increase the sample size, only adding secondary analysis to the original sample).108–112 We excluded 1 paper because it did not include patients,29 1 because it did not include patients with a diagnosis of an anxiety disorder,112 1 because it did not test anxiety as an outcome measure,113 and 1 because the full text was not available.114 Figure 1 summarizes the selection procedure.

Flow chart of study selection. rTMS = repetitive transcranial magnetic stimulation; tDCS = transcranial direct current stimulation.
Overall, 11 studies met our inclusion criteria and were included in the meta-analysis. Study characteristics are shown in Table 1.
Summary of study characteristics used for quantitative analysis
Study quality assessment
Results of the quality assessment are reported in Table 2. We calculated the percentage of high-risk judgments to obtain a quality score for each study. The average quality of the included studies was high to intermediate (range 0% to 42.86%); random sequence generation was the primary source of methodological bias, followed by blinding mode. Most of the studies did not describe randomization procedures, and 2 studies employed a single-blind design.88,120 Three studies87,88,115 reported confusing information about the number of patients excluded from the final sample analyzed.
Risk of bias among included studies
We evaluated reporting bias based on the details reported in the full text, except for 3 studies86,116,121 whose registered protocol was available to check the completeness and consistency of the findings. Of these, Nasiri and colleagues121 did not report analyses and results for some of the preregistered outcome variables, because the report was part of a larger project. Concerning allocation concealment, only Nasiri and colleagues121 received a high-risk judgment because they used cognitive treatment and not sham stimulation as a control condition.
Participant characteristics and inclusion/exclusion criteria
Eleven studies were included in the meta-analysis, involving 154 participants assigned to stimulation groups and 164 to control groups. Participants’ ages ranged from 18 to 65 years; when reported (10 out of 11 studies), participants’ mean age (± SD) was 36.4 ± 6.6 years for the stimulation groups and 36.8 ± 7.2 years for the control groups. In most studies, the number of females was greater than the number of males, and secondary school was the most common education level. Specific participant characteristics from the included studies are reported in Table 3.
Summary of participant characteristics from the included studies
The studies differed in terms of number of stimulation sessions (1–25 sessions), intervention techniques (rTMS, tDCS or iTBS), the presence or absence of concomitant treatments (pharmacological or psychological interventions) and patient diagnoses.
Inclusion and exclusion criteria differed across studies. Participants were typically included if they were in a certain age range, had a specific diagnosis (according to standardized diagnostic manuals such as the Diagnostic and Statistical Manual of Mental Disorders [DSM] and the International Classification of Diseases [ICD]) and had a certain questionnaire score. Depression comorbidity was diagnosed by the authors when patients also fulfilled the criteria for depression (according to DSM standards). Exclusion criteria typically concerned previous psychiatric history (except for the disorder being investigated) and suicidality (Table 4).
Inclusion and exclusion criteria for the included studies
Patient diagnoses
Studies were included if participants received a primary diagnosis of an anxiety disorder, which could be comorbid with depression. Studies in which anxiety was secondary to other conditions (e.g., an organic/neurologic condition, substance use, etc.) were excluded. Participants had a diagnosis of generalized anxiety disorder in 6 of the 11 included studies86,87,116,118,120,121 — combined with insomnia in 1 of the 6118 and combined with MDD in 1 of the 6.121 In 3 studies, participants had panic disorder with or without agoraphobia115,119,122 — combined with MDD in 1 of the 3.119 The last 2 papers included participants with a specific phobia: spider phobia88 and acrophobia.117
Associated therapies
Four of 11 studies88,115,117,121 provided psychological interventions as part of treatment. In the study by Deppermann and colleagues,115 participants took part in 3 group sessions of psychoeducation about panic disorder, which occurred separately from the stimulation sessions. Nasiri and colleagues121 added noninvasive brain stimulation to the last 2 weeks of 12 weekly sessions of a unified protocol123 (the unified protocol is a transdiagnostic treatment for emotional disorders that is aimed at targeting the common features of anxiety and mood disorders using a single psychological treatment), but they did not indicate whether the stimulation was time-locked (e.g., during or immediately before) to the psychological intervention. Notzon and colleagues88 and Herrmann and colleagues117 applied noninvasive brain stimulation before exposure to virtual reality; the interventions occurred in single and double sessions, respectively. In 2 of 11 studies,87,119 individual or supportive psychotherapy was allowed during noninvasive brain stimulation sessions; in 4 of 11 studies,86,116,118,120 psychological interventions were not permitted during noninvasive brain stimulation treatment. One study122 did not report on this factor.
Four of 11 studies88,117,120,121 did not allow medication use during noninvasive brain stimulation treatment; the other 786,87,115,116,118,121,122 reported that stable medication treatment was accepted. Medication stability was defined differently across the studies, ranging from 4 weeks before treatment onset120 to 3 months before (Table 5).116,118
Summary of stimulation protocols details, treatment strategies and associated therapies
Stimulation protocols
Of the 11 included studies, 6 used an rTMS protocol,87,116–119,122 3 a tDCS protocol86,120,121 and 2 an iTBS protocol.88,115 In the rTMS studies, stimulation was applied at 1 Hz in 4 of 6 studies,116,118,119,122 at 20 Hz in 1 study87 and at 10 Hz in 1 study.117 The target region for rTMS was the right dlPFC in 4 of the 6 studies, the right posterior parietal cortex in 1 study118 and the ventromedial prefrontal cortex in 1 study.117 The 2 iTBS protocols were applied over the left dlPFC.88,115 In the 3 tDCS studies, stimulation was delivered with cathodal polarity over the right dlPFC in 2 of 3 studies120,121 and with anodal polarity over the left dlPFC in 1 study.86 Overall, inhibitory protocols (cathodal tDCS, 1 Hz rTMS) were applied over the right dlPFC in 5 of 6 studies; only 1 targeted the right posterior parietal cortex. Facilitatory protocols (iTBS, anodal tDCS and 20 Hz rTMS) were delivered over the left dlPFC in 3 of 5 studies, over the right dlPFC in 1 study (see Figure 2 for a graphical representation of targeted regions) and over the ventromedial prefrontal cortex in 1 study. The stimulation intensity range in TMS studies was between 80% and 110% of the individual rest motor threshold. Magnetic pulses were delivered with figure-8-shaped coils, except for the study by Herrmann and colleagues,117 in which a round coil was used. The tDCS protocols were administered at 2 mA in the 3 studies, with unipolar montages and intracephalic reference in 1 of 3 studies86 and a deltoid reference in 2 of 3 studies.120,121 Stimulation duration ranged from 10 to 30 minutes. See Table 5 and Table 6 for details.

Type of stimulation and target regions in included studies. Red dots indicate excitatory stimulation protocols (i.e., anodal tDCS, iTBS and high-frequency rTMS); blue dots indicate inhibitory stimulation (i.e., cathodal tDCS and low-frequency rTMS). The size of the dots correspond to the number of studies that applied an excitatory or inhibitory protocol over a specific region: 5 studies applied inhibitory stimulation protocols over the right dorsolateral prefrontal cortex, 3 studies applied excitatory stimulation protocols over the left dorsolateral prefrontal cortex, 1 study applied an excitatory stimulation protocol over the right dorsolateral prefrontal cortex, 1 study applied an inhibitory stimulation protocol over the right posterior parietal cortex, and 1 study applied an excitatory stimulation protocol over the ventromedial prefrontal cortex. Brain images were obtained from www.nitrc.org. iTBS = intermittent theta burst stimulation; rTMS = repetitive transcranial magnetic stimulation; tDCS = transcranial direct current stimulation.
Summary of stimulation protocol, statistical analyses, main results and additional groups and measures (part 1 of 2)
Control condition
The presence of a control condition was an inclusion criterion for our meta-analysis. For 10 of 11 studies, this consisted of a sham condition. In 1 study,121 the control group did not receive a sham stimulation; instead, they underwent unified protocol treatment. For rTMS studies, sham stimulation was induced by varying the coil inclination at 90° with respect to the stimulation site in 4 of 8 studies.87,88,115,122 In the other 4 studies,116,118,121,124 experimenters used a sham coil, which had the same appearance and produced the same noise as the real coil. Among the 3 tDCS studies, 1 applied the typical sham tDCS protocol:86 the stimulation was on for the first 30 seconds, inducing the same skin sensation as the real stimulation;125 Movahed and colleagues120 did not report their sham protocol parameters. Nasiri and colleagues121 did not have a sham condition; instead, they included a control group in which participants took part in cognitive treatment.
Nine of the 11 studies were double-blind, with both experimenters and participants blind to participants’ assigned condition. Two of the 11 studies88,120 used a single-blind design, in which only participants were blind to their stimulation group. In 4 of 11 studies, participants’ blinding was checked using specific questionnaires.88,115,117,119
Outcome measures
As noted above, we chose 3 outcome measures: an anxiety measure centred on the specific disorder investigated in each study, which was reported in 10 of 11 studies (all but Dilkov and colleagues87); a general anxiety measure, investigating general anxiety symptoms, reported in 9 of 11 studies (all but Notzon and colleagues88 and Herrmann and colleagues117); and a measure of depression, which was included in 7 of 11 studies (depression questionnaires were not included in 4 studies88,115,117,118).
Specific anxiety measure
The specific anxiety outcome measure included scores from a heterogeneous pool of clinical validated questionnaires, depending on the specific disease investigated. For panic disorder, 2 of 3 studies119,122 administered the Panic Disorder Severity Scale126 and 1 study115 administered the Panic and Agoraphobia Scale.127 For the specific phobia studies, Notzon and colleagues88 used the German version of the Spider Phobia Questionnaire,128,129 and Herrmann and colleagues117 used the German translation of the Acrophobia Questionnaire130 anxiety subscale. For generalized anxiety disorder, the Penn State Worry Questionnaire131 was used for 2 of 6 studies,116,120 the Generalized Anxiety Disorder Questionnaire132 was used for 1 study,121 the Lipp Inventory of Stress Symptoms for Adults133 was used for 1 study86 and the Pittsburgh Sleep Quality Index,134 investigating insomnia symptoms, was used for 1 study.118 The final generalized anxiety disorder study87 did not include a disorder-specific questionnaire; it was not included in the specific anxiety disorders analysis.
General anxiety measure
For 8 of 9 studies we included the HAM-A,135 a 14-item clinical interview targeting somatic and psychic anxiety symptoms. For 1 of 9 studies121 we included the BAI,136 a 21-item self-report questionnaire focusing on the somatic symptoms of anxiety occurring over the past week. Notzon and colleagues88 did not include a general anxiety measure; this study was not included in the analysis of general indexes of anxiety.
Depression measure
Five of 7 studies87,116,118–120 used the HAM-D,137 a 21-item (only the first 17 aligned with the total score) clinical interview targeting somatic and neurovegetative aspects of depression. Two of 7 studies86,121 used the Beck Depression Inventory,138 a 21-item self-report questionnaire investigating the cognitive and affective dimensions of depression (for a comparison between HAM-D and the Beck Depression Inventory, see Brown and colleagues139). When both the clinical and the self-report measures of general anxiety or depression were reported, we considered only the clinician-administered version.
Meta-analysis
Anxiety-specific disorders
Ten of 11 studies reported scores for specific anxiety disorder scales (Table 1). We ran a meta-analysis on these studies to compute the global effect of noninvasive brain stimulation on the reduction of anxiety-specific symptoms compared to a sham intervention. The random-effects model showed a significant medium effect of noninvasive brain stimulation on patients’ symptom improvement compared to pre/post sham scores (overall SMD −0.49, 95% CI −0.83 to −0.14; p = 0.006; see Table 7 for complete results and Figure 3 for a forest plot).
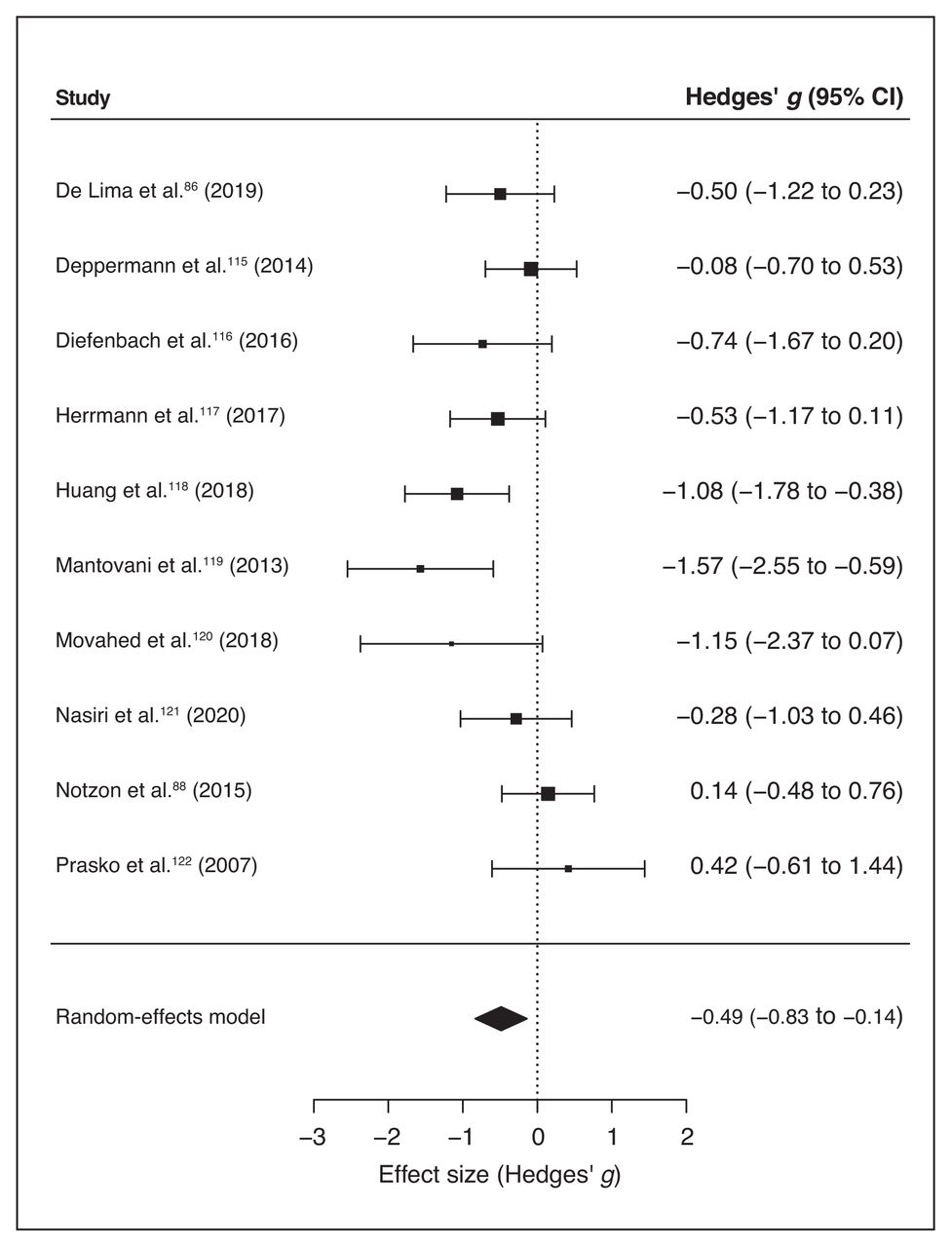
Forest plot of the effect size of noninvasive brain stimulation on continuous specific anxiety questionnaire scores. CI = confidence interval.
Summary of the results of the 3 meta-analyses
Q statistics and I2 suggested high heterogeneity between studies (Table 7); this may have been due to differences in methodological factors across studies. The inclusion of moderators — namely the duration of treatment (computed as the number of stimulation sessions), the stimulation technique applied (iTBS, rTMS, tDCS), the protocol type (excitatory v. inhibitory), the target region (left v. right dlPFC; Huang and colleagues118 targeted a different region, so we did not include it when analyzing the moderation effect of the target region) and comorbid depression (presence v. absence) — was not significant (all p > 0.13; see Table 8 for moderators’ statistical results).
Results of the moderation analysis for specific and general anxiety scores and depression scores
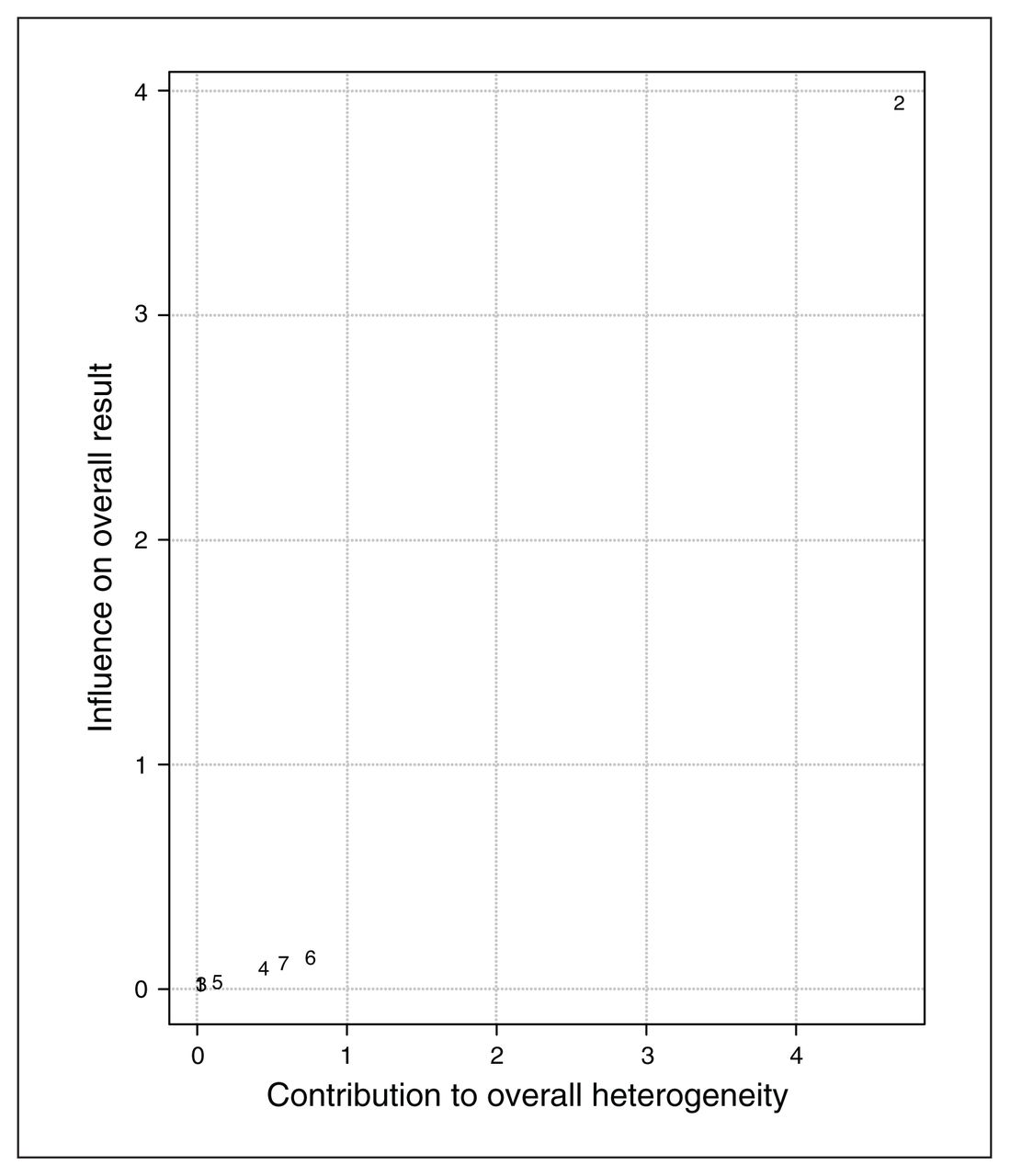
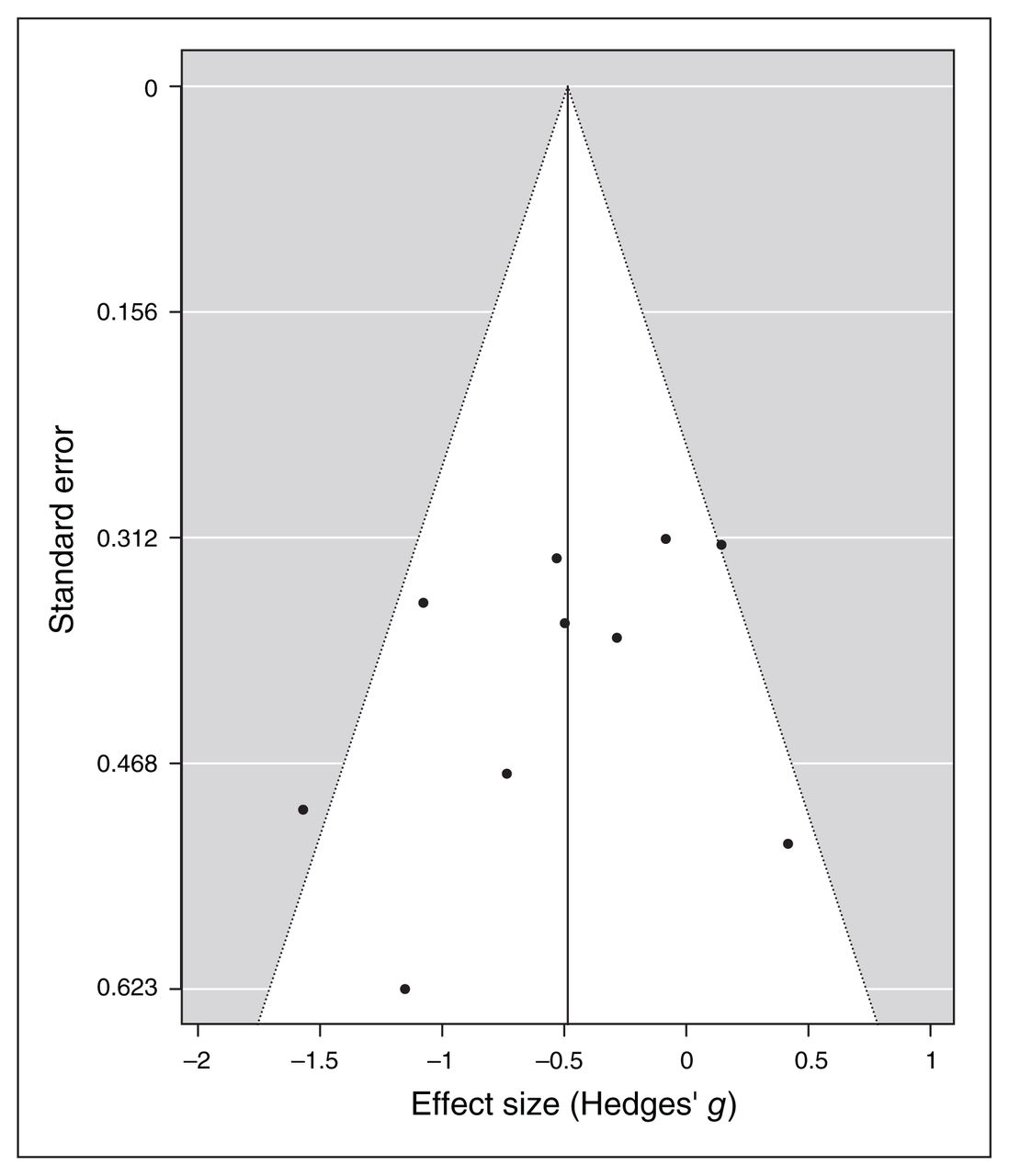
Baujat plot inspection140 (Figure 4) suggested that study 8119 greatly contributed to the heterogeneity of the meta-analysis. Nevertheless, testing for a possible outlier influence of the included studies in the results91 showed that no study differed significantly from the rest of the data (Table 7). In terms of publication bias, the funnel plot (Figure 5) showed no asymmetry according to both Egger’s regression test (z = −1.21; p = 0.23) and the rank correlation analysis (Kendall’s tau = −0.29; p = 0.29).

Baujat plot of study distribution in terms of heterogeneity for continuous specific anxiety questionnaire scores. On visual inspection, study 8119 seemed to contribute most to the statistical heterogeneity of the included studies.
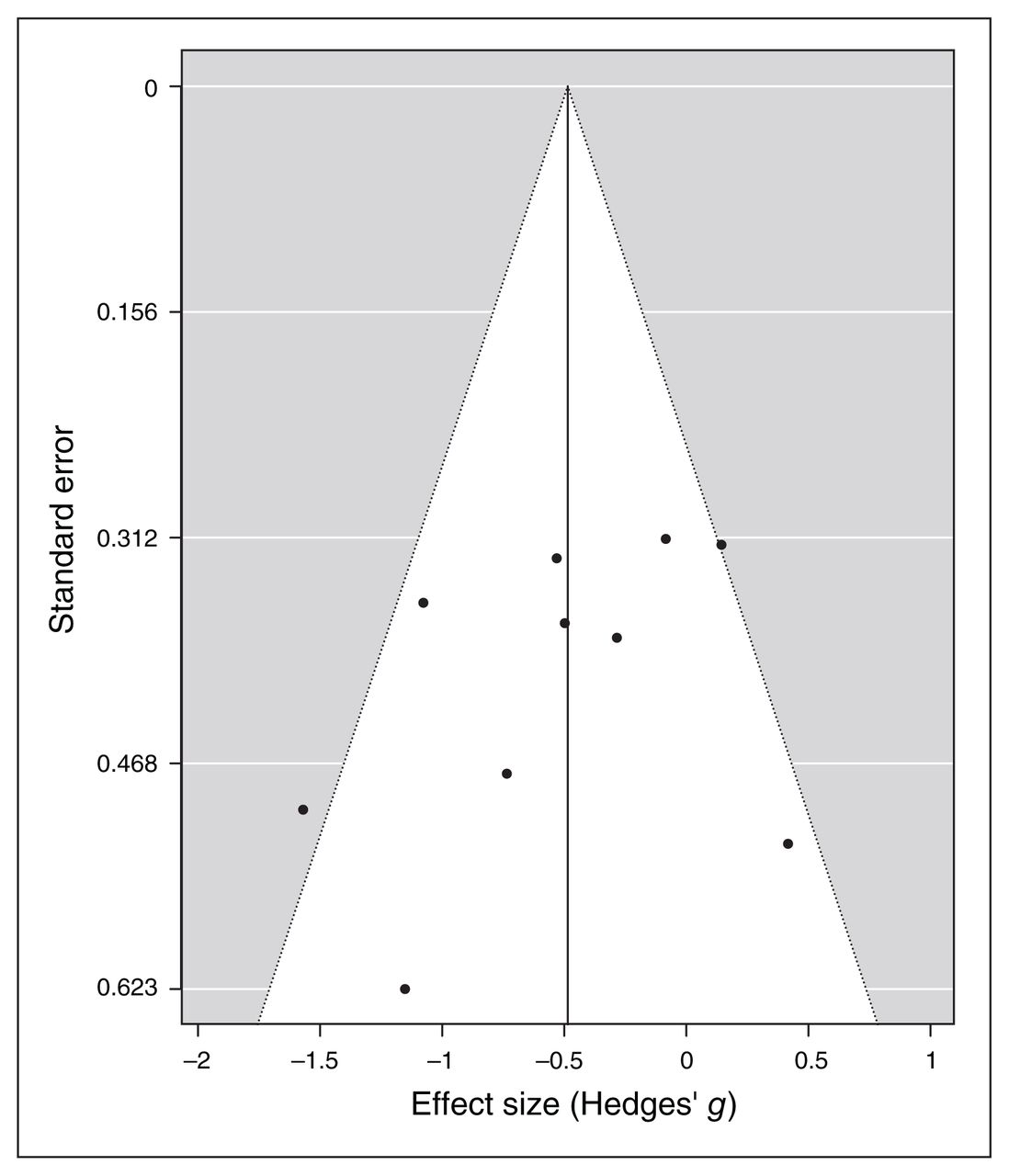
Publication bias assessed by funnel plot for continuous specific anxiety questionnaire scores.
General anxiety indexes
Along with the specific anxiety measures, 9 of the 11 included studies reported pre/post general BAI and HAM-A scores for the stimulation and sham groups, we ran a separate meta-analysis for these scales. Similar to the specific anxiety symptoms, the random effect model for general anxiety indexes showed a significant medium to large effect of noninvasive brain stimulation on the reduction of general anxiety scores compared to sham treatment (overall SMD −0.81, 95% CI −1.45 to −0.18; p = 0.012; see Table 7 for complete results and Figure 6 for a forest plot).
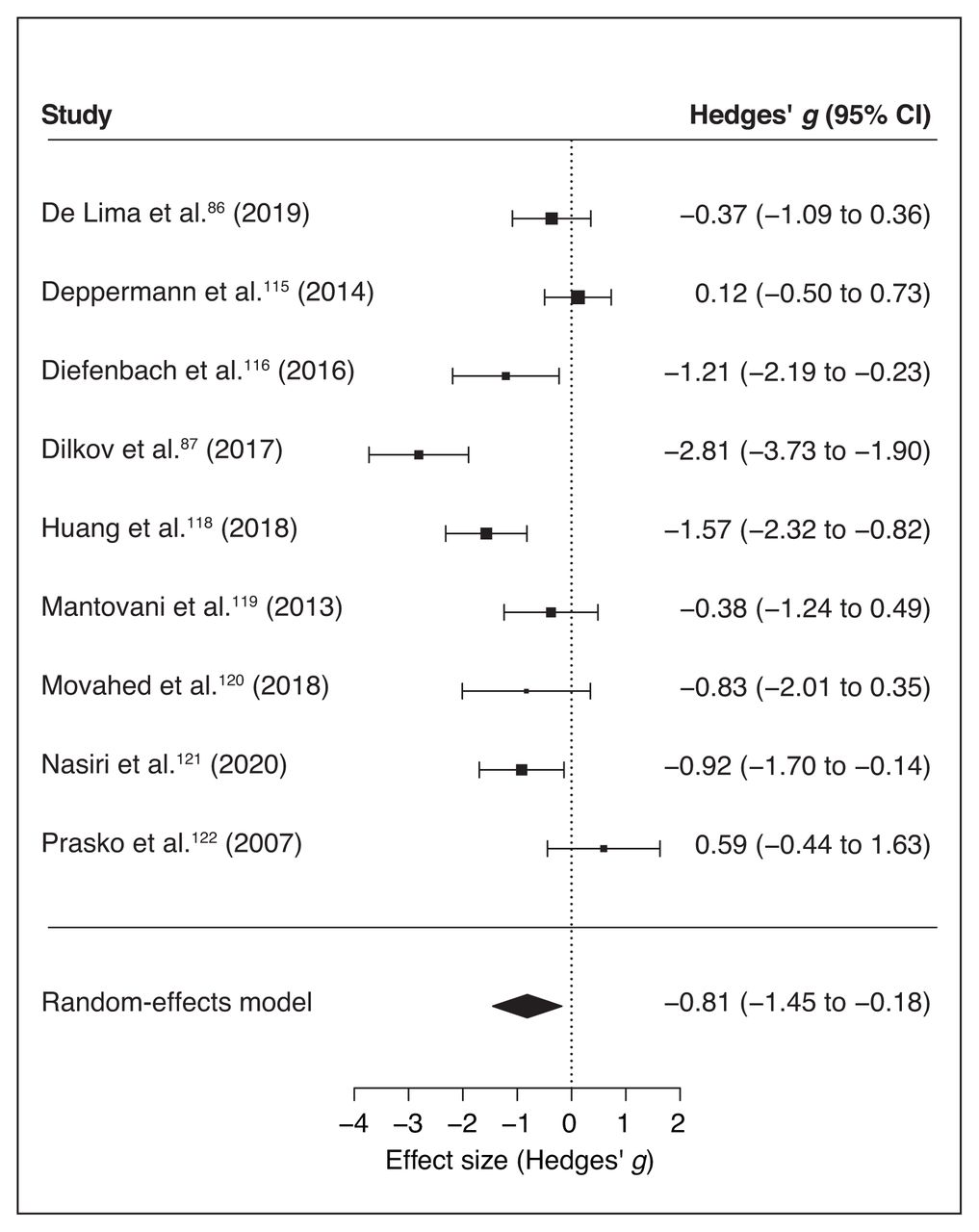
Forest plot of the effect size of noninvasive brain stimulation on continuous general anxiety questionnaire scores. CI = confidence interval.
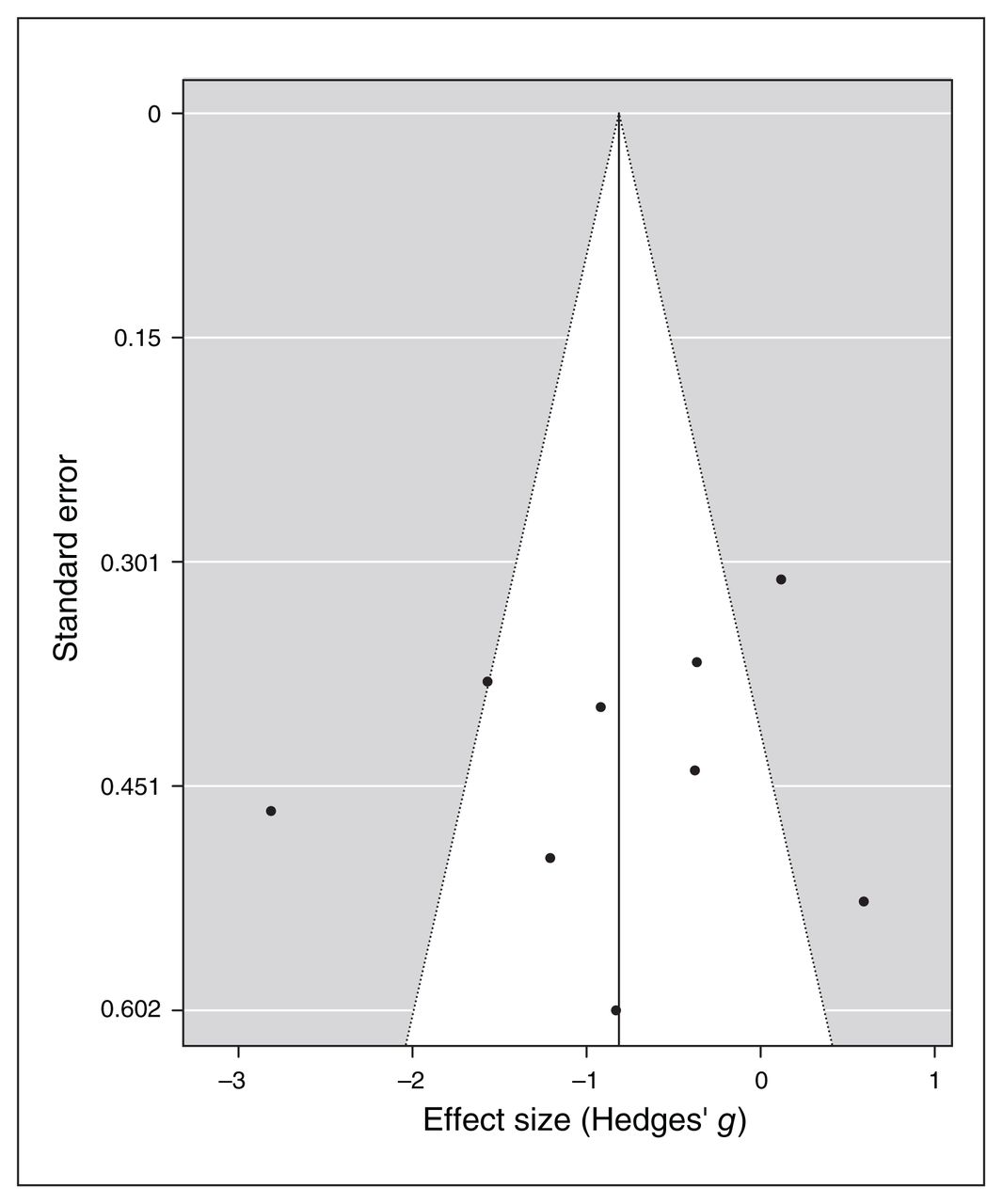
For specific symptoms, I2 and Q statistics suggested high heterogeneity across studies, and a Baujat plot suggested that study 387 was the main source of variance (Figure 7). Indeed, the influence test highlighted this study as an outlier (Table 7). Therefore, we re-ran the random-effects model excluding this study from the pool, and the global effect of noninvasive brain stimulation on the reduction of general anxiety scores remained significant (overall SMD −0.57, 95% CI −1.06 to −0.07; p = 0.024; see Table 7 for complete results). No other study was a significant outlier. Therefore we proceeded with the moderation analysis using the original set of 9 studies. The inclusion of moderators in the model was not significant (p > 0.19, Table 8). Funnel plot asymmetry (Figure 8) was nonsignificant for Egger’s regression test (z = −0.31, p = 0.76) and rank correlation analysis (Kendall’s tau = −0.17; p = 0.61).
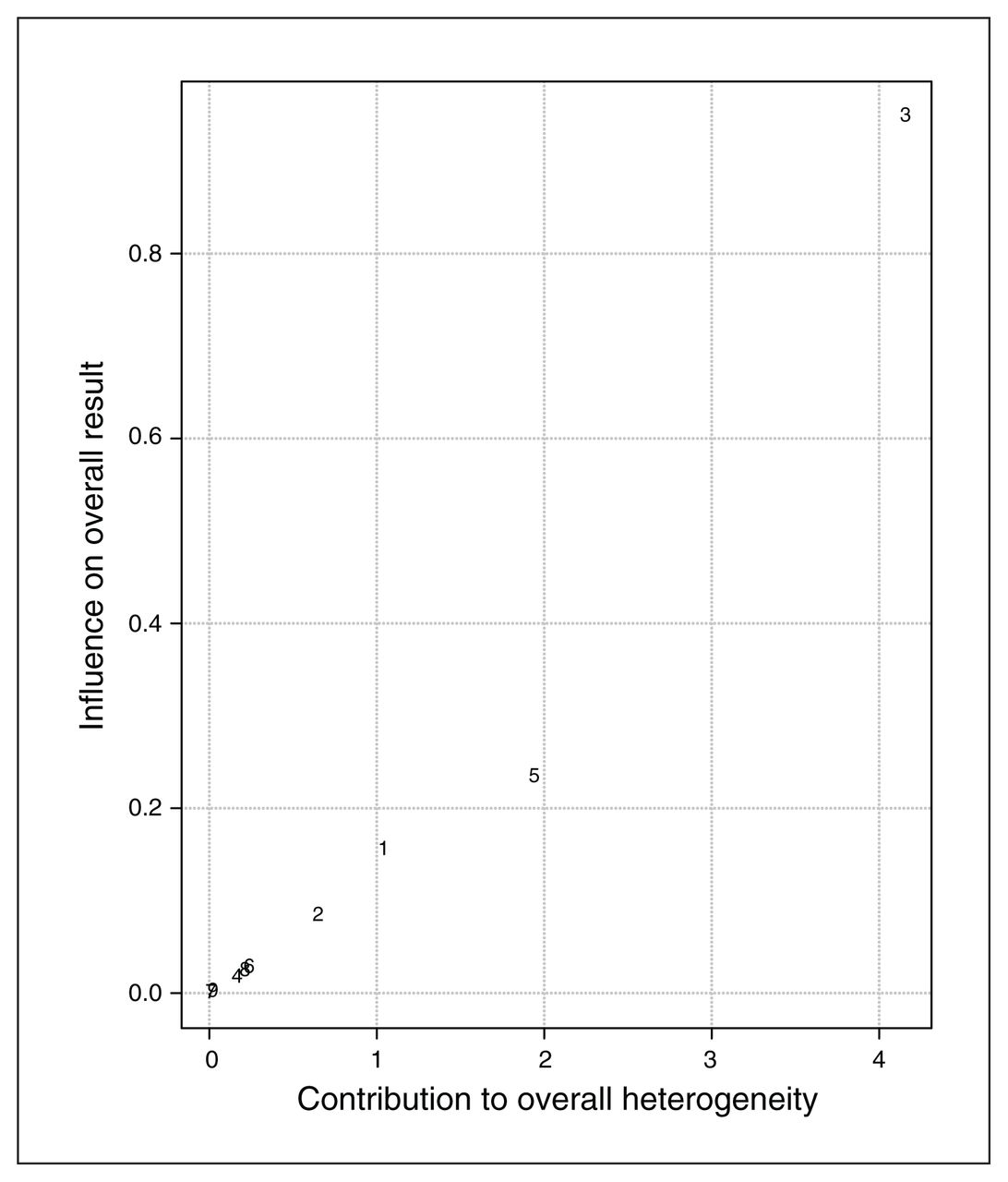
Baujat plot of study distribution in terms of heterogeneity for continuous general anxiety questionnaire scores. On visual inspection, study 387 seemed to contribute most to the statistical heterogeneity of the included studies.

Publication bias assessed by funnel plot for continuous general anxiety questionnaire scores.
Depression scales
Seven of the final pool studies reported depression scale scores (Table 1) before and after the intervention. The random-effects model reported a significant global effect of noninvasive brain stimulation in reducing the scores on the depression inventories compared to sham interventions (overall SMD −0.98, 95% CI −1.62 to −0.35; p = 0.002; see Table 7 for the complete results and Figure 9 for a forest plot).

Forest plot of the effect size of noninvasive brain stimulation on continuous depression questionnaire scores. CI = confidence interval.
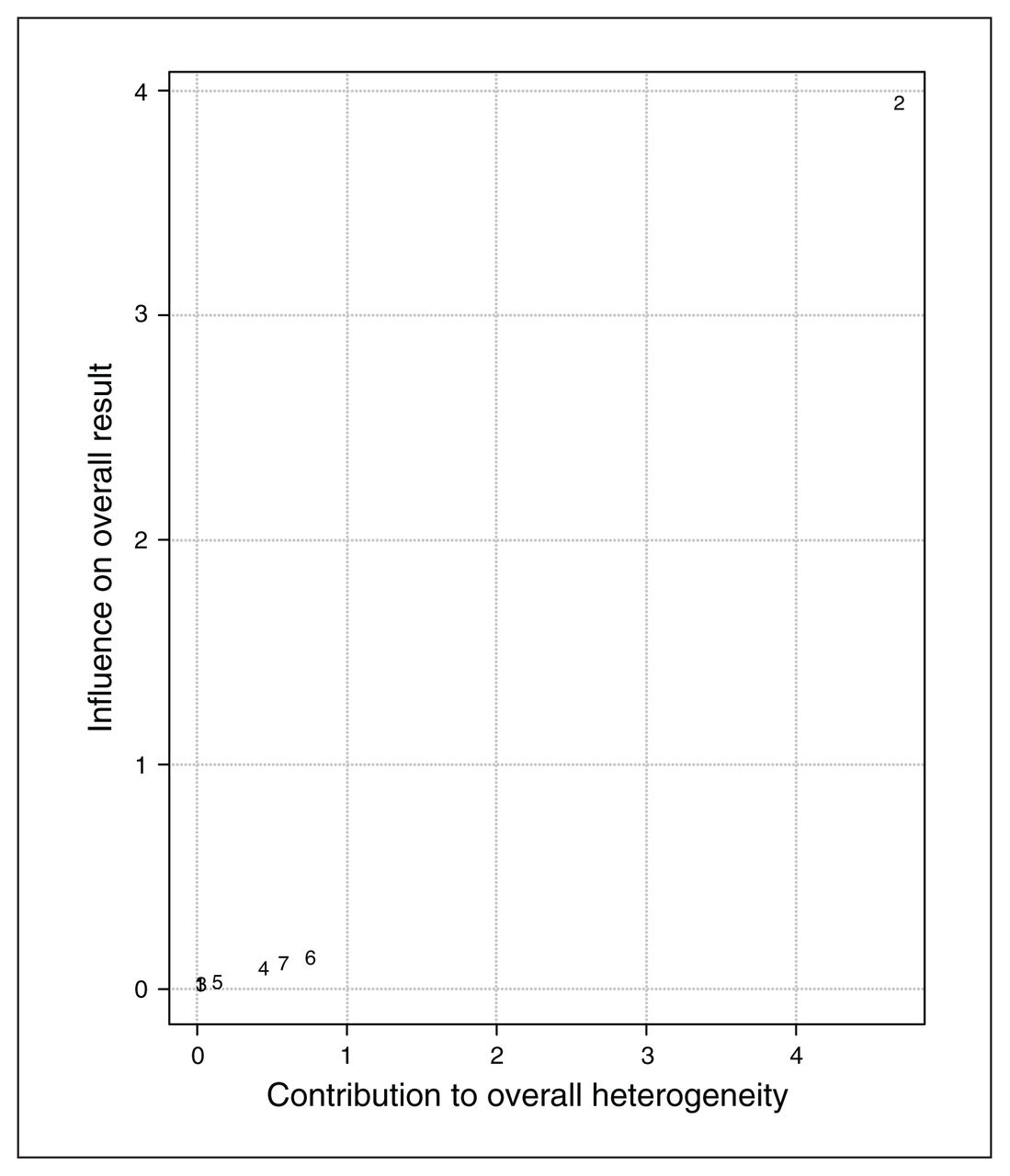
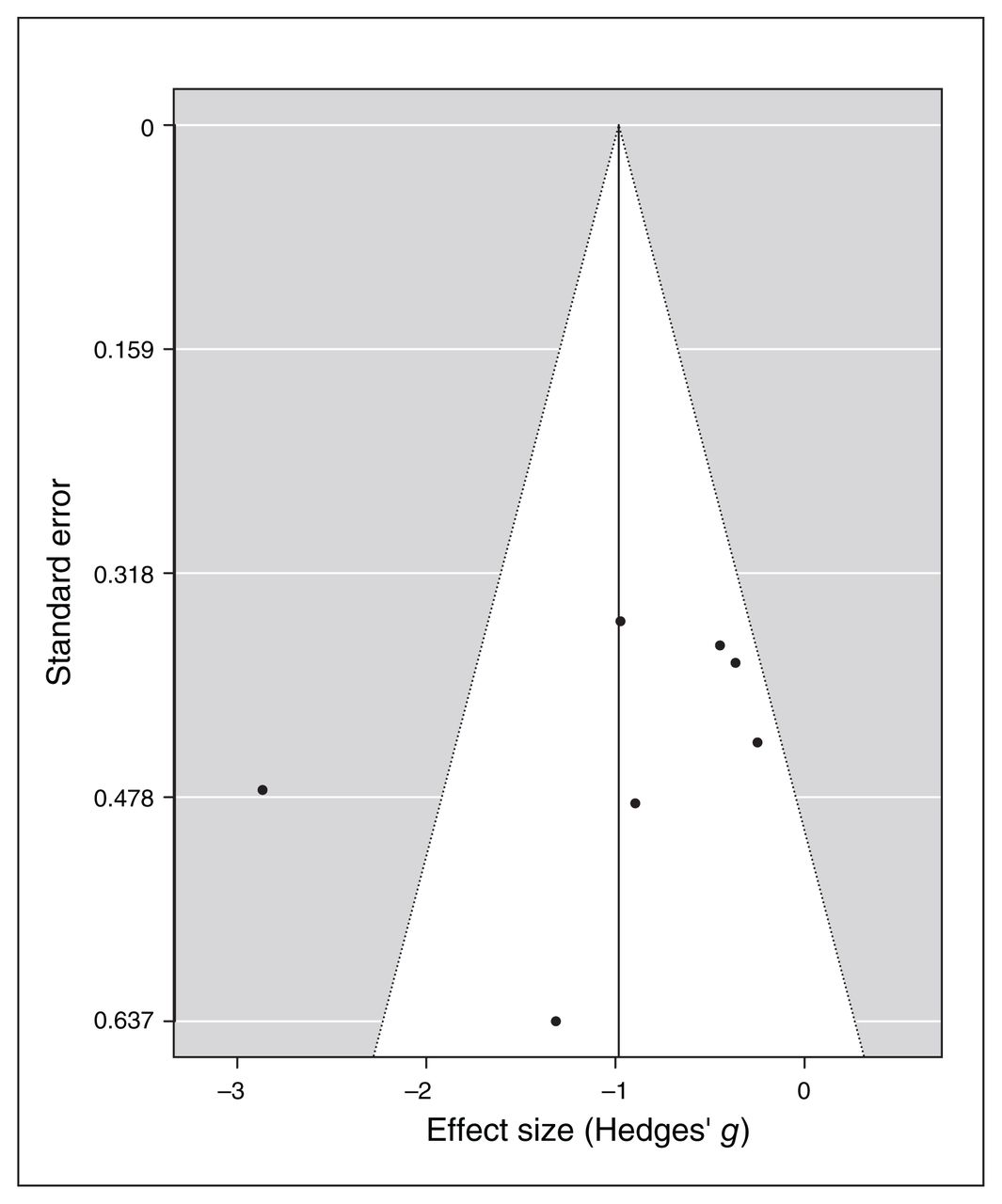
I2 and Q statistics suggested high heterogeneity across studies. The Baujat plot (Figure 10) suggested that study 287 was the main source of variance. The influence test identified this study as an outlier (Table 7). Still, even excluding this study from the meta-analysis the model highlighted a significant effect of noninvasive brain stimulation on reduction of depression scores (overall SMD −0.64, 95% CI −0.98 to −0.31; p < 0.001; see Table 7 for complete results). No further study resulted in an outlier from the influence analysis. Therefore, we proceeded with the moderation analysis using the original set of 7 studies. Analysis of moderators indicated a trend toward significance for the number of stimulation sessions on the reduction of depression symptoms (QM1 = 3.1, p = 0.08), with a higher reduction when the number of sessions increased. We found no effect for the presence of comorbidity in depression scores after treatment (p = 0.16). Funnel plot asymmetry (Figure 11) was nonsignificant for both the Egger’s regression test (z = −0.8, p = 0.43) and the rank correlation analysis (Kendall’s tau = −0.07; p > 0.99).
Baujat plot of study distribution in terms of heterogeneity for continuous depression questionnaire scores. On visual inspection, study 287 seemed to contribute most to the statistical heterogeneity of the included studies.

Publication bias assessed by funnel plot for continuous depression questionnaire scores.
Discussion
Rationale and description of the study procedure
Over the last few decades, the high rate of nonresponders to conventional treatment and low adherence to pharmacological interventions because of significant adverse effects has led to increasing demand for novel and complementary treatment approaches, including noninvasive brain stimulation. The effectiveness of rTMS in depression is well recognized and its clinical use is accepted worldwide;40 as well, recent expert guidelines for tDCS have pointed in the same direction.66 And yet, to date very little evidence has been available for the efficacy of noninvasive brain stimulation in anxiety disorders65–67,141 because of a low number of studies specifically investigating this topic.
We conducted a systematic review and quantitative analysis of the effectiveness of noninvasive brain stimulation in ameliorating the clinical symptoms of anxiety disorders. We included peer-reviewed original studies written in English in the present work. Given the importance of comparison with a placebo or control treatment, we included only studies that compared real stimulation with sham or control conditions.
Overall, 11 articles met our inclusion criteria. Studies differed in terms of the specific anxiety disorder they investigated: 10 of 11 studies (all but Dilkov and colleagues87) reported using disorder-specific questionnaires (e.g., the Panic Disorder Severity Scale in panic disorder). As well, 9 of 11 studies (all but Notzon and colleagues88 and Diefenbach and colleagues116) included a general anxiety measure (HAM-A or BAI). Therefore, we ran 2 separate meta-analyses for anxiety symptoms. The first included the results from a specific disorder questionnaire used in each study. The second included the results from a general anxiety questionnaire (HAM-A or BAI; the clinician-administered HAM-A was preferred when available). Finally, 7 studies86,87,116,118–121 also included scores on a depression scale (HAM-D or Beck Depression Inventory), the focus of our third meta-analysis. It is well known that anxiety and depression are often comorbid and share some commonalities in the neural substrate involved. For this reason, we wanted to investigate whether noninvasive brain stimulation was useful in reducing symptoms of depression as well as anxiety.
Main effect of noninvasive brain stimulation on anxiety and moderation analysis
Our findings highlighted a significant medium effect of stimulation in decreasing anxiety scores compared to control conditions, suggesting that noninvasive brain stimulation can be useful in reducing symptoms of anxiety in patients. This effect was significant for both the disorder-specific and general anxiety measures, in line with the high correlation found between the 2 measures of anxiety (0.6), and might have been because of changes in symptoms that are shared by the various anxiety disorders. Crucially, the effect was not likely to have been influenced by publication or reporting bias. In line with previous systematic reviews35 and meta-analyses,72,73 we also acknowledge the limitations of these results, which are based on a restricted sample of studies but a relatively large pool of patients (318 in total).
We included only representative moderators in our moderation analyses because of the small number of studies in our analysis. For example, only 2 studies targeted the right parietal region PPC118 and the ventromedial prefrontal cortex;117 all of the others targeted the dlPFC. Therefore, we ran the moderation analysis comparing stimulation of the left versus the right dlPFC. The analysis of moderators did not highlight any significant predictors, possibly because of the limited number of available studies. Only the number of stimulation sessions revealed a trend toward significance: depressive symptoms decreased for studies that included more sessions, in line with another recent meta-analysis.142 The influence of number of sessions in modulating depressive symptoms is debated but still controversial. Some studies and meta-analyses have reported a nonsignificant effect of dosage on symptom modulation,143,144 and others have suggested that at least 20–30 sessions (or more) are required for optimal effects.145,146
Q statistics and I2 suggested high heterogeneity across studies, probably because of methodological differences across the selected works. Indeed, protocols varied with respect to participant diagnosis and treatment, the inclusion of associated therapies and protocol-specific parameters, target brain regions and the duration of the intervention. Specifically, participant diagnosis included generalized anxiety disorder (combined with insomnia or major depression), panic disorder (with or without agoraphobia and sometimes with comorbid major depression) and specific spider phobia. There was also heterogeneity in participants’ ability to combine noninvasive brain stimulation with a medication or psychological treatment. In 3 studies88,120,121 participants were not allowed to follow a drug therapy; in the other, they could continue their treatment or follow a new one.115 In the latter situation, a time interval was established before starting noninvasive brain stimulation treatment; the interval varied across studies but was at least 3 weeks. Only 4 protocols88,115,117,121 included a psychological intervention.
Combination of psychological intervention and neurostimulation
Psychological and stimulation interventions were not always combined in the same sessions; in other words, they were not sequentially or simultaneously time-locked.41 Indeed, in 1 study,115 participants took part in 3 group sessions of panic disorder psychoeducation, separate from the noninvasive brain stimulation. In another study,121 tDCS was applied in the last 2 weeks of an emotional disorder psychological treatment process (unified protocol), but the authors did not specify whether tDCS was applied before, during or after treatment. Only Notzon and colleagues88 and Herrmann and colleagues117 provided a combined approach to a specific phobia, delivering iTBS before virtual reality exposure. Notzon and colleagues88 did not report any changes as a result of the single-session intervention, but in the study by Herrmann and colleagues,117 the 2-session treatment led to a reduction in anxiety symptom scores. As previously highlighted by other researchers (see Sathappan and colleagues41 for a recent review), the effect of combining behavioural or cognitive interventions with noninvasive brain stimulation is a gap in neuropsychiatric literature research. Indeed, it is well known that the effects of noninvasive brain stimulation are state dependent, meaning that the state of the stimulated regions during stimulation has a great influence on its effects on cortical excitability57,147–149 and behaviour.150–152 Moreover, converging evidence has suggested that both stimulation and psychotherapy can modulate brain connectivity,153,154 pointing to the possible importance of time-locking brain stimulation and behavioural engagement to investigate the possibility of maximizing their effects. A similar approach has been applied with stroke patients in the neurorehabilitation field, combining noninvasive brain stimulation with motor and speech training (for recent reviews, see Breining and Sebastian155 and Pruski and Cantarero156). In neuropsychiatric disorders, the investigation of combined interventions is still in its infancy,41,157 even for the treatment of depression, which has received more research attention.41,144 In anxiety disorders, Heeren and colleagues113 combined the attentional bias modification technique with anodal and sham tDCS to reduce the bias for threat in patients with social anxiety. The study had a crossover design; participants performed only 2 sessions — a sham one and a real one — and the authors reported a significant reduction in bias in the real stimulation condition compared to the sham stimulation. Segrave and colleagues158 combined tDCS with simultaneous cognitive treatment (cognitive control therapy) in patients with MDD in 5 consecutive daily sessions. Real and sham tDCS led to equal improvements in depression symptoms after the fifth session of the protocol; however, effects were maintained at 3-week follow-up in only the group assigned to the real stimulation. In patients with schizophrenia, brain stimulation has been combined with cognitive remediation in an attempt to improve the cognitive deficits typical of the disease, but this has produced mixed results.159 There is evidence from experimental, behavioural and clinical research suggesting that the coupling of noninvasive brain stimulation with a concomitant treatment might enhance efficacy compared to each intervention alone. However, results are scarce and controversial, and this topic needs further investigation.
Noninvasive brain stimulation to treat anxiety
Most of the noninvasive brain stimulation studies in our review included a TMS intervention — either rTMS87,116–119,122 or iTBS.88,115 Only 3 studies86,120,121 used a tDCS intervention. This choice was in line with knowledge about the treatment of depression, in which rTMS is considered a useful method for treating drug-resistant depression and because rTMS has stronger spatial resolution than tDCS.160 However, in a combined approach, tDCS can be a convenient option, with fewer exogenous distractions related to rTMS-induced noise and fewer muscular contractions. The latter can be annoying or painful, especially when electrodes are applied to the prefrontal regions, the regions typically targeted in treatments we reviewed.
Recently, in addition to tDCS and rTMS, deep TMS has gained ground in treating the symptoms of obsessive–compulsive disorder161,162 and MDD (see Gellersen and Kedzior163 for a meta-analysis), and it has received US Food and Drug Administration clearance for both treatments. This technique uses the principles of TMS but delivers current through a specially designed H-coil that can modulate cortical excitability up to 6 cm in depth, reaching not only cerebral cortex activity but also the activity of deeper neural circuits.164 To our knowledge, no previous studies have investigated deep TMS for anxiety disorders, and no articles about this technique appeared in our literature search combining “transcranial magnetic stimulation” or “TMS” with the 5 anxiety categories. However, given that we did not systematically search the term “deep TMS,” we combined the key words “deep TMS” with each of the anxiety disorders in the 3 previously investigated databases. PubMed and Scopus research reported no results, and Web of Science search produced 3 results (the 3 results came from the combination of “deep TMS” and “generalized anxiety disorder”;165 “deep TMS” and “specific phobia”;166 and “deep TMS” and “social anxiety disorder”167): a nonoriginal study,165 a study in animals166 and a study in patients with depression.167 The lack of studies evaluating deep TMS for anxiety disorders reflects the general limited number of studies investigating noninvasive brain stimulation and anxiety disorders compared to other psychiatric conditions and points to the importance of shedding light in this field.
Comorbidity of anxiety and depression
With respect to the clinical comorbidity of anxiety and depressive disorders, our results highlighted the efficacy of noninvasive brain stimulation in reducing depression scores compared to the control condition, an effect that was not merely shown in studies in which comorbidity was formally diagnosed in the sample population. This finding was in line with previous studies that investigated the effectiveness of rTMS in reducing anxiety symptoms during the treatment of patients with depression. In one of the largest studies, Chen and colleagues168 investigated the efficacy of left-dlPFC high-frequency, right-dlPFC low-frequency and sequential bilateral rTMS (i.e., high-frequency left dlPFC followed by low-frequency right dlPFC) in a sample of 697 participants. The stimulation protocols showed the overall efficacy of the 3 protocols in reducing anxiety and depressive symptoms without indicating that one protocol had a stronger therapeutic effectiveness over the other. In another study, Clarke and colleagues103 analyzed data from a sample of 248 patients with treatment-resistant depression, of whom 172 had 1 or more comorbid anxiety disorders. rTMS was applied using 1 Hz to the right dlPFC or a sequential bilateral protocol (10 Hz over the left dlPFC and 1 Hz over the right dlPFC). Interestingly, rTMS reduced anxiety levels in patients with and without a formal anxiety diagnosis, as shown by a significant reduction in HAM-A scores in both subgroups. Similarly, in our sample 9 of 11 interventions targeted the left or right dlPFC; only 2 studies117,118 targeted a different site, namely the right posterior parietal cortex and the ventromedial prefrontal cortex, respectively. Crucially, when applied over the right hemisphere (dlPFC or posterior parietal cortex) stimulation was inhibitory (except for Dilkov and colleagues,87 who applied an excitatory protocol over the right dlPFC), with cathodal tDCS or low-frequency (1 Hz) rTMS. Over the left dlPFC, all studies applied excitatory protocols as iTBS and anodal tDCS. This choice was in line with previous knowledge related to the neural underpinning of anxiety disorders, which suggests that the left dlPFC is typically hypoactive in anxiety disorders, and the right dlPFC seems hyperactive.33,34,169 The overlap between the targeted regions and inhibition or excitation protocols explains the reported efficacy of noninvasive brain stimulation in reducing both anxiety and depression scores compared to control conditions. Indeed, although international guidelines and the US Food and Drug Administration approval recommend the application of excitatory (high-frequency rTMS, deep TMS or anodal tDCS) stimulation over the left dlPFC, it is known that noninvasive brain stimulation can also influence brain excitability through interhemispheric projections. Based on this idea, a change in excitability in one hemisphere — also induced by exogenous stimulation such as noninvasive brain stimulation — might induce indirect changes in the excitability of the other hemisphere, and eventually in behavioural outcomes. Such an effect has been reported for cognitive and motor tasks involving the prefrontal and frontal regions170–172 and for neurorehabilitation, especially involving post-stroke patients.173,174
The latter result is exciting and paves the way to specifically investigating the phenomenological overlapping of depression and anxiety disorders. Indeed, the fact that the stimulation of a similar brain network modulates both anxiety and depression symptoms, and some antidepressant drugs do the same (serotonin/adrenaline reuptake inhibitors show an effectiveness in treating both disorders) suggests a similarity in the neurochemical basis of the 2 syndromes. A recent study by Maggioni and colleagues175 specifically investigated neural commonalities and differences between anxiety and depression using structural MRI. Although this study was preliminary, its findings suggested that the clinical similarities between major depression and anxiety might rely on common prefrontal alterations involving left orbitofrontal thinning, while frontotemporal abnormalities are traceable in MDD and parietal abnormalities are specific to panic and social anxiety disorders.
It is interesting to note that the prefrontal regions are generally linked to emotional processing and regulation,31,176–178 which are known to be at the basis of the development and maintenance of anxiety and depression. For instance, studies in healthy participants have suggested that stimulation of the left dlPFC has positive effects on modulating several cognitive, emotional and neural processes that are relevant to anxiety.29,113,179,180 (See Stein and colleagues181 for a systematic review of the effects of tDCS in anxiety disorders or anxious behaviours in healthy participants.)
A final comment should be made about the outcome measures. The included studies used scores on validated questionnaires as outcome measures. However, only 1 study88 investigated psychophysiological measures in addition to questionnaire results, evaluating skin conductance level and heart rate variability. The authors found no differences in skin conductance level but they did find a modulation in heart rate variability in the iTBS group versus the sham group, independent of the participant sample (patients v. healthy individuals). It is not usual to measure implicit psychophysiological measures as indicators of treatment effectiveness when applying noninvasive brain stimulation.35 However, such measures might be an index not only for assessing treatment improvement, but also for dosing the intervention in a flexible way and as predictors of treatment outcomes. For example, in a previous study with veterans affected by posttraumatic stress disorder, the baseline startle response to virtual reality combat-related scenes was predictive of clinical outcomes: higher startle responses predicted greater changes in symptom severity at the end of the 6 weeks of treatment.182
Limitations
Research investigating the relationship between noninvasive brain stimulation and anxiety disorders is still in an embryonic state. Overall, just a few studies targeting patients with anxiety disorders are available; many authors have focused instead on healthy participants with a high trait of anxiety. For the studies that did include a clinical sample, only a few protocols investigated the efficacy of noninvasive brain stimulation at a group level. Moreover, the inclusion of a sham or control condition for comparison with the stimulation condition is not standard in research, despite the fact that the placebo effect of noninvasive brain stimulation techniques is well-known in both participants and experimenters, highlighting the importance of applying double-blind procedures.183,184 Future studies should also move in the direction of coupling noninvasive brain stimulation with behavioural or cognitive interventions, investigating whether combined treatment is more effective than monotherapy. Another crucial point about the efficacy of noninvasive brain stimulation protocols is based on sex. A limitation of the present study was the lack of a regression analysis including sex as a moderator. Unfortunately, none of the included studies reported outcome scores separately based on participants’ sex.
Conclusion
Although our findings are preliminary, they suggest that noninvasive brain stimulation can be effective in decreasing anxiety and depressive symptoms in anxiety disorders, paving the way for treatment protocols that include noninvasive brain stimulation. Further research is needed to optimize the protocols in terms of duration, location, intensity and technique, and to define potential interindividual differences in response to neuromodulation induced by noninvasive brain stimulation.55
Footnotes
Funding: A. Vergallito was supported in part by a 2019 NARSAD Young Investigator Grant, Brain & Behavior Research Foundation.
Competing interests: None declared.
Contributors: A. Vergallito, A. Galluci, A. Pisoni and L. Romero Lauro designed the study. A. Vergallito, A. Gallucci, A. Pisoni and M. Punzi acquired and analyzed the data, which G. Caselli, G. Ruggiero, S. Sassaroli and L. Romero Lauro interpreted. A. Vergallito, A. Galluci, A. Pisoni and M. Punzi wrote the article, which G. Caselli, G. Ruggiero, S. Sassaroli and L. Romero Lauro reviewed. All authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
- Received March 29, 2021.
- Revision received May 23, 2021.
- Accepted July 2, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools


