

Article Figures & Tables
Figures
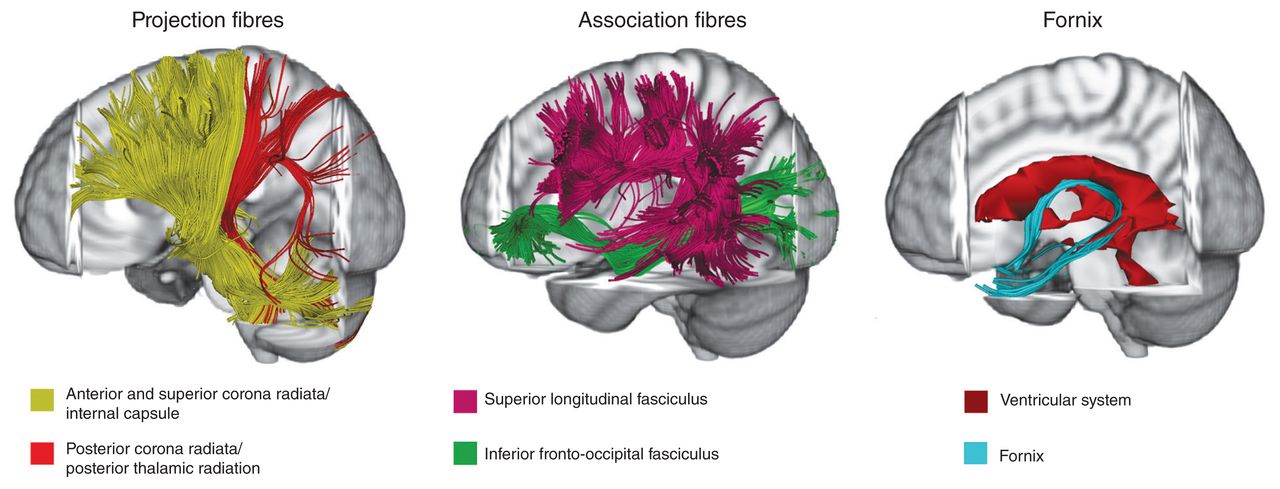
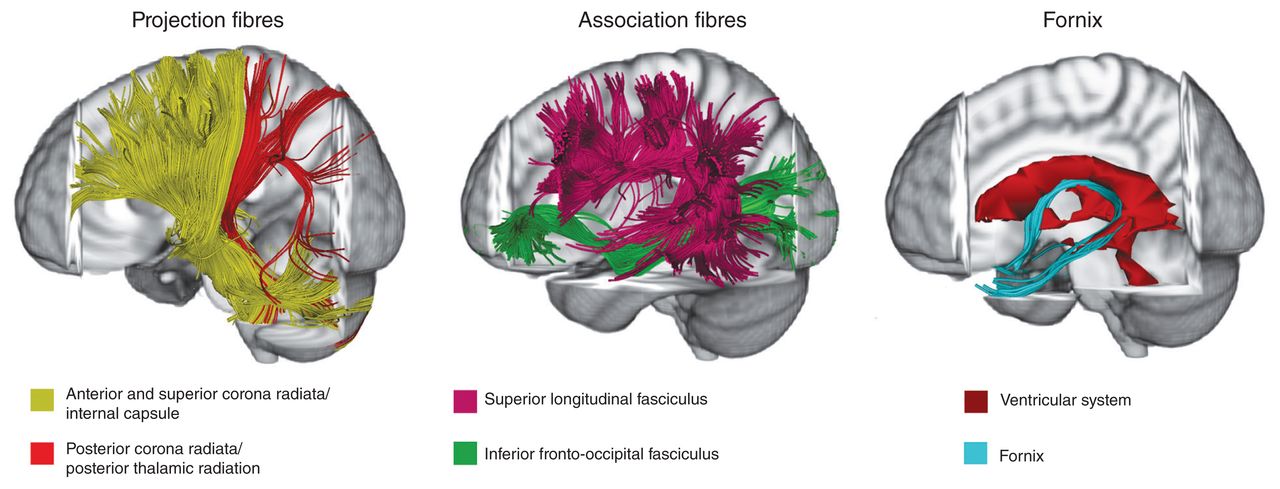
- Fig. 1
Main white matter tracts affected in eating disoders. This figure represents white matter tracts mainly altered in anorexia nervosa and bulimia nervosa studies on a representative subject (tractographic reconstruction). See Table 2 for specific details of tract alterations. Three-dimensional fibre tractography was performed using the diffusion tensor imaging track module provided in MedINRIA software (ASCLEPIOS Research Team, Sophia Antipolis Cedex, v 1.9.0 France, www-sop.inria.fr/asclepios). For more details on white matter fibre reconstruction, see Wakana and colleagues, (36) Mori and colleagues (60) and Nagae and colleagues. (61) Projection fibres Association fibres
Tables
- Table 1
Sample characteristics of DTI studies and evaluation procedures for hydration state
Study Participants, n Age, yr mean ± SD BMI, kg/m2 mean ± SD Eating disorder duration, yr mean ± SD Evaluation of hydration status Cross-sectional studies in participants with anorexia nervosa Frank et al. (44) AN = 19 15.4 ± 1.4 16.2 ± 1.1 NR Supervised food and fluid intake HC = 22 14.8 ± 1.8 21.3 ± 1.9 — Gaudio et al. (45) AN = 14 15.7 ± 1.6 16.2 ± 1.2 0.4 ± 0.1 Voxel-based morphometry analysis of grey matter, white matter and cerebrospinal fluid volumes HC = 15 16.3 ± 1.5 21.1 ± 1.9 — Hayes et al. (46) AN = 8 35 ± 11 NR 16.25 ± 6.4 NR HC = 8 36 ± 9 — — Hu et al. (47) AN = 8 17.6 ± 2.2 14.3 ± 1.3 0.9 ± 6.2 At least 1 week of supervised meals and hydration HC = 14 19.1 ± 3.1 20.1 ± 1.7 — Kaufmann et al. (37) AN = 25 22.84 ± 4.75 13.83 ± 1.33 16.04 ± 2.63 Supervised food and fluid intake; volumes of the third and lateral ventricles as covariates; correction for free water at the voxel level HC = 25 23.36 ± 3.35 21.07 ± 1.93 — Kazlouski et al. (38) AN = 16 23.9 ± 7 16.5 ± 1 7.5 ± 8 Supervised food and fluid intake; exclusion criteria: gross electrolyte or complete blood count abnormalities HC = 17 25.1 ± 4 21.5 ± 1 — Nagahara et al. (48) AN = 17 23.8 ± 6.68 13.6 ± 1.3 4.93 ± 4.9 Electrolytes and complete blood count HC = 18 26.2 ± 5.6 19.9 ± 2.0 — Travis et al. (49) AN = 15 16.6 ± 1.4 16.0 ± 1.2 1.4 ± 1.0 NR HC = 15 17.1 ± 1.3 21.4 ± 2.1 — Via et al. (50) AN = 19 28.37 ± 9.55 17.03 ± 1.09 6.5 ± 6.0 Supervised food and fluid intake HC = 19 28.63 ± 8.58 21.09 ± 1.80 — Vogel et al. (51) AN = 22 15.03 ± 1.60 15.36 ± 1.08 1.20 ± 1.30 Urine specific gravity ANd = 9* 14.76 ± 2.30 17.45 ± 1.43 NR HC = 21 15.17 ± 1.28 20.34 ± 2.59 — Cross-sectional and longitudinal studies in participants with anorexia nervosa von Schwanenflug et al. (52) AN = 56 15.9 ± 2.9 14.7 ± 1.3 1.2 ± 1.8 Urine specific gravity ANf = 44 15.7 ± 2.3 18.7 ± 1.1 NR HC = 60 16.2 ± 2.9 20.6 ± 2.4 — Cross-sectional studies in participants with current and past anorexia nervosa Frieling et al. (53) AN = 12 26.84 ± 6.94 15.18 ± 1.39 NR NR ANrec = 9 27.44 ± 5.32 19.31 ± 1.39 NR HC = 20 24.80 ± 2.60 19.60 ± 0.94 — Pfuhl el al. (39) AN = 35 16.1 ± 2.8 14.70 ± 1.31 NR Urine specific gravity ANrec = 35 22.5 ± 3.0 21.09 ± 1.91 NR HC v. AN = 31 16.4 ± 2.6 20.75 ± 2.98 — HC v. ANrec = 31 22.5 ± 2.9 21.34 ± 2.18 — Cross-sectional studies in participants recovered from anorexia nervosa Bang et al. (54) ANrec = 21 27.6 ± 5.1 20.4 ± 1.7 2.8 ± 2.3 — HC = 21 26.1 ± 4.7 21.8 ± 1.8 — Shott et al. (55) ANrec = 24 30.25 ± 8.13 20.83 ± 2.37 5.90 ± 5.21 — HC = 24 27.42 ± 6.28 21.64 ± 1.26 — Yau et al. (56) ANrec = 12 28.7 ± 7.9 21.2 ± 1.5 5.7 ± 5.2 — HC = 10 26.7 ± 5.4 22.0 ± 1.1 — Longitudinal studies in participants with restrictive eating disorders Olivo et al. (57) RED = 12 15.3 ± 1.5 18.7 ± 2.9 0.7 ± 0.46 NR REDf = 12 16.4 ± 1.5 21.1 ± 2.7 NR HC = 24 14.1 ± 1.0 20.6 ± 2.6 — Cross-sectional studies in participants with bulimia nervosa He et al. (58) BN = 28 21.32 ± 6.11 21.95 ± 2.13 5.9 ± 6.4 — HC = 28 20.61 ± 6.12 22.18 ± 2.14 — Mettler et al. (59) BN = 20 25.2 ± 5.3 22.59 ± 5.69 6.2 ± 5.3 — HC = 21 27.5 ± 6.6 21.55 ± 1.19 — AN = anorexia nervosa; ANd = anorexia nervosa at discharge; ANf = anorexia nervosa at follow-up; ANrec = anorexia nervosa, recovered; BN = bulimia nervosa; BMI = body mass index; DTI = diffusion tensor imaging; HC = healthy control; NR = not reported; RED = restrictive eating disorder; rEDf = restrictive eating disorder at follow-up; SD = standard deviation.
↵* An exploratory longitudinal study was also conducted.
- Table 2
Scanning methods, main results and main clinical interpretation from DTI studies in patients with eating disorders (part 1 of 5)
Study Methods Main results Main clinical interpretation Field strength/ sequence No. of directions Tool Type of analysis DTI measures Atlas Cross-sectional studies in participants with anorexia nervosa Frank et al. (44) 3 T/NR 25 NordicICE VBA FA, ADC Hutchins Lower FA values in left fornix, bilateral CG, right forceps major, right superior and left posterior CR. Higher FA values in left SLF, bilateral anterior CR and bilateral IFOF. Higher ADC values in left fornix, right CC, right corticospinal tract, right posterior CR, bilateral corticopontine tract and bilateral SLF. Altered white matter integrity may be related to impaired taste, reward and emotional processing. Gaudio et al. (45) 1.5 T/ SE, EP 12 FDT TBSS FA, MD, AD, RD JHU white matter labels Lower FA values in left anterior and superior CR, left SLF, fornix and body of the CC. Lower AD values in the left and right SLF, left superior and anterior CR, and the external capsule, posterior limb of internal capsule and posterior thalamic radiation (including optic radiation) of the right hemisphere. White matter alterations may be related to altered cognitive flexibility and body-image disturbances. Hayes et al. (46) 3 T/DSE, EP 60 FDT, 3D slicer eXtended streamline tractography, ROI (subcallosal cingulate), ROI (fornix crus, PTR/SLF, CC splenium, ALIC, anterior CG, IFOF, posterior CG, CC genu) Fibre connections, FA, AD, RD DTI-81 atlas Higher connectivity from the subcallosal cingulate white matter in the prefrontal and left parieto-occipital cortices, and lower connectivity in the thalamus identified by deterministic multitensor tractography. Lower FA values, associated with lower AD and higher RD, were found within the anterior limb of the internal capsule, right anterior CG, and left fornix crus and IFOF. Higher RD values were found in the anterior limb of the internal capsule and IFOF. White matter tract alterations may be related to altered processing of affective stimuli, self-perception and interoception in anorexia nervosa. Hu et al. (47) 3 T/SS, EP 25 DTI Studio, SPM 8, in-house made VBA, ROI (based on group comparison results) FA — VBA: significant decrease in FA maps in the left superior frontal gyrus, medial frontal gyrus, anterior cingulate cortex, middle frontal gyrus, inferior frontal gyrus, thalamus and bilateral insula. ROI: significantly positive correlations between the mean FA value of the left inferior frontal gyrus, insula and thalamus and BMI in patients with anorexia nervosa. White matter alterations may be involved in pathophysiology of anorexia nervosa. Kaufmann et al. (37) 3 T/SENSE, EP 64 FDT† TBSS FA (ROI) Juelich Histological Atlas ROI-based approach: fornix. No FA values differences between anorexia nervosa patients and controls after correction for free water. FA values alterations of forniceal fibres seem significantly biased by partial volume effects in anorexia nervosa. Kazlouski et al. (38) 3 T/NR 25 DTI Studio VBA, ROI (based on group comparison results) FA, ADC Mori (2005) Lower FA values in bilateral fimbria-fornix region, fronto-occipital fasciculus and posterior CG. Higher ADC values in frontoparietal and parietal–occipital white matter (with uncorrected threshold). Altered white matter integrity in brain areas that integrate emotion, reward and cognitive behaviours may be related to pathophysiology of anorexia nervosa. Nagahara et al. (48) 3 T/SS, SE, EP 32 FDT TBSS FA, MD Johns Hopkins University Lower FA values in cerebellum. Higher MD values in fornix. Fornix and cebebellum white matter alterations may be related to the pathophysiology of anorexia nervosa. Travis et al. (49) 3 T/DSE, EP 96 mrDiffusion AFQ FA* R1* — Lower and higher FA values in 6 tracts (18 examined) and 1 subdivision of the CC (8 examined). Lower R1 in 6 cerebral tracts (18 examined) and 5 subdivisions of the CC (8 examined). White matter changes seem to be related to changes in myelin content. Via et al. (50) 1.5 T/SS, SE, EP 25 FDT TBSS FA, MD, RD,* AD* Mori (2007) Lower FA values in the parietal part of the left SLF, associated with higher MD and RD values. Higher MD values in the fornix associated with lower FA and higher RD and AD values. Altered white matter integrity may be related to body image distortion, altered weight regulation and reward-processing alterations. Vogel et al. (51)† 3 T/ DSE, EPI 30 FDT TBSS, ROI (based on group comparison results) FA, MD, RD, AD — Higher FA values in the bilateral superior CR, anterior CC, anterior and posterior thalamic radiation, anterior and posterior limb of internal capsule, and left inferior longitudinal fasciculus. Altered FA values were mainly related to lower RD and MD values but not to altered AD values. Exploratory longitudinal study showed similar results with a greatly reduced level of significance. Altered FA values could be related to an acute state of anorexia nervosa. Cross-sectional and longitudinal studies in participants with anorexia nervosa von Schwanenflug et al. (52) 3 T/NR 32 FDT TBSS FA, MD, AD, RD Juelich Histological Atlas Baseline: Lower FA and higher MD, AD and RD values in the body of CC. Longitudinal: No differences between follow-up patients and controls. Higher FA and lower AD, MD and RD v. baseline in the fornix, bilateral optic radiation and CC. Reduced FA and increased MD and RD v. baseline in right corticospinal tract. Altered microstructural properties in people with anorexia nervosa normalized rapidly during nutritional therapy. These findings underline that structural brain alterations associated with the disorder are highly dynamic and more likely to represent consequences of starvation state than pre-existing or white matter degeneration. Cross-sectional studies in participants with current and past anorexia nervosa Frieling et al. (53) 3 T/ SS, SE, EP 15 Native VBA FA Talairach Daemon Lower FA values in the posterior thalamic radiation bilaterally and the left mediodorsal thalamus in patients with anorexia nervosa compared with controls. Additional regional lower FA values in parts of the posterior CR bilaterally, the left middle cerebellar peduncle, and in parts of the left SLF. A volume-of-interest-based post hoc analysis of these regions (posterior thalamic radiation bilaterally and the left mediodorsal thalamus) showed no significant differences between patients with acute anorexia nervosa and patients recovered from anorexia nervosa. FA value alterations may contribute to altered processing of the body image and impairments in cognitive domains. Pfuhl el al. (39) 3 T/SE 30 TRACULA Tractography, cluster analysis FA, MD, RD, AD — Tractography: No differences in FA, MD, RD and AD between the acute anorexia nervosa subjects and controls. Supplementary cluster analysis: no significant differences. No significant differences in both the main and supplementary cluster analyses between people recovered from anorexia nervosa and controls. White matter microstructure is preserved in patients with acute anorexia nervosa and patients recovered from anorexia nervosa. Cross-sectional studies in participants recovered from anorexia nervosa Bang et al. (54) 3 T/SS, EP 32 FDT TBSS, voxel-wise correlation FA, MD, AD, RD — No significant differences between patients with anorexia nervosa and controls in white matter microstructure (FA, MD, RD and AD values). White matter alterations observed during the acute phase of anorexia nervosa are reversible in long-term recovered patients. Shott et al. (55) 3 T/NR 25 FDT Probabilistic tractography, ROI (taste-reward circuit), TBSS Fibre connections, FA Mori (2005) Seed-based approach: taste-reward-related white matter tracts. Higher white matter connectivity between bilateral insula regions and ventral striatum, left insula and middle orbitofrontal cortex, and right insula projecting to gyrus rectus and medial orbitofrontal cortex. Seed-based FA analysis: Lower FA values in some tracts between insula subregions and ventral striatum and orbitofrontal cortex regions. Whole-brain FA analysis: lower FA values in the anterior CR, external capsule and cerebellum including the corticopontine tract, CC, anterior thalamic radiation, inferior and middle cerebellar peduncle, as well as inferior fronto-occipital and uncinate fasciculi. White matter alterations suggest altered connectivity within taste-reward pathways and may impair reward circuit functions that drives food intake. Yau et al. (56) 3 T/SS, EP 55 FDT TBSS FA, MD, AD,* RD* — Lower MD values in 6 clusters encompassing parietal, CG and frontal white matter tracts. Lower LD and/or RD in these regions. No FA values alterations between patients recovered from anorexia nervosa and controls. Lower MD values may be related to premorbid behavioural traits (harm avoidance and heightened concern for mistakes) through an exaggerated cognitive control. Longitudinal studies in participants with restrictive eating disorders Olivo et al. (57) 3 T/EP 48 FDT TBSS FA, MD, AD, RD ICBM-DTI-81 white matter labels Analysis at baseline: Lower FA values in the CC (genu, body and splenium), anterior and superior CR bilaterally, right posterior CR, posterior thalamic radiation and right tapetum. Higher RD values in the aforementioned tracts. Longitudinal analysis: no differences between follow-up patients and baseline controls, or between baseline and follow-up patients. White matter alterations may have a role in the alteration in food-related cognitive processing present in adolescents with restrictive eating disorders. Cross-sectional studies in participants with bulimia nervosa He et al. (58) 3 T/ SS, SE, EP 25 FDT TBSS FA, MD, AD, RD Johns Hopkins University A priori hypothesis analysis: lower FA values in the forceps minor and major, SLF, IFOF, anterior thalamic radiation, corticospinal tract, uncinate fasciculus and CG in both hemispheres. Exploratory analysis (RD): Higher RD values in many of the same tracts: forceps minor and major, left SLF, IFOF, anterior thalamic radiation, corticospinal tract and CG. These results suggest that white matter is affected in bulimia nervosa. Altered white matter tracts may have a role in the persistence of impaired self-regulation in bulimia nervosa. Mettler et al. (59) 3 T/NR 25 NordicICE VBA FA, ADC Hutchins and Atlas of Brain Function Orrison Lower FA values in the bilateral CR, CC, right subinsula, and right fornix. Higher ADC values in the bilateral CR, CC, inferior fronto-occipital and uncinate fasciculi. Bulimia nervosa is associated with white matter alterations that may contribute to altered trait anxiety, mood disturbance and altered reward processing. AD = axial diffusivity; ADC = apparent diffusion coefficient; AFQ = automated fibre quantification; ALIC = anterior limb of internal capsule; BMI = body mass index; CC = corpus callosum; CG = cingulum; CR = corona radiata; DSE = double psin echo; DTI = diffusion tensor imaging; EP = echo planar; EPI = echo-planar imaging; FA = fractional anisotropy; IFOF = inferior fronto-occipital fasciculus; LD = longitudinal diffusivity; MD = mean diffusivity; NR = not reported; PTR/SLF = junction of the posterior thalamic radiation/superior longitudinal fasciculus; R1 = relaxation rate; RD = radial diffusivity; ROI = region of interest; SE = spin echo; SENSE = sensitivity encoding; SLF = superior longitudinal fasciculus; SS = single-shot; TBSS = tract-based spatial statistics; VBA = voxel-based analysis.
↵* Investigated in regions that showed group differences in fractional anisotropy or mean diffusivity.
↵† An exploratory longitudinal study was also conducted.

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.