

Abstract
Background Disturbances in gain and loss processing have been extensively reported in adults with addiction, a brain disorder characterized by obsession with addictive substances or behaviours. Previous studies have provided conflicting results with respect to neural abnormalities in gain processing in addiction, and few investigations into loss processing.
Methods We conducted voxel-wise meta-analyses of abnormal task-evoked regional activities in adults with substance dependence and gambling addiction during the processing of gains and losses not related to their addiction (mainly monetary). We identified 24 studies, including 465 participants with substance dependence, 81 with gambling addiction and 490 healthy controls.
Results Compared with healthy controls, all participants with addictions showed hypoactivations in the prefrontal cortex, striatum and insula and hyperactivations in the default mode network during gain anticipation; hyperactivations in the prefrontal cortex and both hyper- and hypoactivations in the striatum during loss anticipation; and hyperactivations in the occipital lobe during gain outcome. In the substance dependence subgroup, activity in the occipital lobe was increased during gain anticipation but decreased during loss anticipation.
Limitations We were unable to conduct meta-analyses in the gambling addiction subgroup because of a limited data set. We did not investigate the effects of clinical variables because of limited information.
Conclusion The current study identified altered brain activity associated with higher- and lower-level function during gain and loss processing for non-addiction (mainly monetary) stimuli in adults with substance dependence and gambling addiction. Adults with addiction were more sensitive to anticipatory gains than losses at higher- and lower-level brain areas. These results may help us to better understand the pathology of gain and loss processing in addiction.
Introduction
Addiction refers to a situation in which substances or activities become the major focus of a person’s life and cause physical or mental harm to the person with the addiction or to other people, a result of the obsession with the addictive substances or behaviours and the exclusion of other activities. Substance dependence is characterized by problematic substance use (e.g., alcohol, cocaine or cannabis),1 which may induce changes in the brain and give rise to physical and psychological disturbances.2,3 In 2019, 35 million people worldwide were estimated to have substance dependence.4 Globally, 4.2% and 1.3% of disease burden5 were attributable to alcohol and drug use, respectively.6 Similar to substance dependence, gambling addiction is an addictive behaviour associated with morbidity and harm. The 12-month prevalence for gambling addiction among adults ranges from 0.1% to 6.0% worldwide.7 Gambling addiction is associated with suicidal ideation and suicide attempts, which result from risk factors such as financial difficulties and depression.8 As well, people with gambling addiction have high rates of comorbid substance dependence.9 Given that addictions such as substance dependence and gambling addiction lead to distress and harm, it is crucial to understand their neural pathophysiology.
Gain and loss processing (or reward and loss processing) refer to the ability to learn from rewarding or undesirable stimuli by assigning specific values to the objects or actions in our environment10 and using that information to guide future behaviours. Disturbances in gain processing — and to a lesser extent, loss processing — have been extensively reported in substance dependence11 and gambling addiction.12 Most experimental paradigms for gain and loss processing require participants to make responses to gain rewards (not related to the addiction, such as money gain or visual erotic rewards) and avoid losses, and to allow for the analysis of different processing phases, such as the anticipation and outcome periods. To control for irrelevant factors such as visual processing of the stimuli and motor processing during responses (i.e., button pressing), researchers usually compare gain or loss trials to neutral trials in which participants have no gain or loss. Such gain– or loss–neutral contrasts permit the analysis of valence-related (i.e., gain or loss) task activation by theoretically making valence the most salient difference among the conditions.13
To date, neuroimaging techniques — especially functional MRI (fMRI) — have been widely used to reveal altered gain and loss processing in adults with substance dependence and gambling addiction.14,15 The neural basis underlying gain and loss processing involves several brain regions, including the prefrontal cortex (PFC), the ventral striatum and the anterior cingulate cortex.16,17 Previous studies have revealed both hyper-and hypoactivity in reward-related regions during both the expectation and receipt of non-drug (mainly monetary) gains in people with addiction compared to healthy controls. Some researchers have observed hypoactivation of the ventral striatum in people with cocaine addiction during both gain and loss anticipation,18 and hypoactivation of the inferior prefrontal gyrus in smokers during gain outcome notification.19 However, other researchers have reported enhanced activation of the ventral striatum in people with alcohol addiction during gain anticipation,20 enhanced activity in the ventromedial PFC in smokers during loss anticipation19 and enhanced activation of the ventral striatum in cannabis-dependent patients during loss outcome notification.21 Similarly, people with gambling addiction have demonstrated diminished activity in the ventral striatum, the ventromedial PFC and the insula during anticipation of both gain and loss,22 as well as diminished activation of the PFC in response to monetary gain and loss outcomes.23 However, gambling addiction has also been associated with enhanced activity in the right ventral striatum during loss anticipation,24 and enhanced activity in the bilateral ventral striatum and left orbital frontal cortex during gain outcome notification.25 In addition, some researchers have found no significant differences between people with addiction and healthy controls. For example, Bjork and colleagues26 found that people with alcohol addiction and healthy controls both showed similar activation patterns in the ventral striatum during gain and loss anticipation for monetary rewards.
To unravel these inconsistent findings (i.e., both hyper- and hypoactivity in reward-related regions during gain and loss processing compared to healthy controls), researchers have been trying to investigate neural abnormalities in addiction from the perspective of meta-analysis.27 Meta-analysis is a statistical process for synthesizing data from multiple independent studies, calculating an overall effect.28 By conducting meta-analyses, Luijten and colleagues27 revealed altered brain activity in people with addiction compared to healthy controls during the anticipation and outcome receipt of monetary rewards, further confirming these results separately in people with substance dependence and gambling addiction. They showed that people with substance dependence and gambling addiction both exhibited attenuated striatal activity compared to healthy controls during gain anticipation, but that people with substance dependence showed enhanced activity in the ventral striatum and people with gambling addiction showed reduced activity in the dorsal striatum during gain outcome. This was an interesting and valuable meta-analysis, and it provided some directions for further investigation. First, it synthesized findings only for gain-related phases, not loss-related phases. Although gain and loss processing seem to capture overlapping neural mechanisms in the healthy population, especially during the anticipation phase,29 how these 2 processes are impaired in people with addiction is as yet unclear. It is likely that they undergo distinct changes in the brain, because gains and losses are valued differently30 and they are assigned different weights when people make decisions.31 Specifically, although altered gain processing may give rise to misrepresentations of rewards (e.g., hypersensitivity to addiction-related rewards according to incentive sensitization theory32,33), impaired loss processing may or may not show the same effect on the evaluation of punishments. Therefore, investigating alterations in loss processing for people with addiction is as important as understanding gain processing. Second, some studies included in the meta-analysis contrasted gain trials with neutral trials, and others contrasted gains directly with losses. This mix of gain–neutral contrasts (20 data sets) and gain–loss contrasts (5 data sets) in a single meta-analysis27 makes it difficult to gain insight into brain-activity alterations for these 2 processes with opposing valences.34,35 Third, because this meta-analysis focused primarily on activation of the striatum, findings from some region-of-interest (ROI) analyses were also included. Findings may be biased because of the ROI choices, and inferences from these findings should be treated with caution.
Overall, based on the studies mentioned above, our metaanalysis aimed to integrate brain imaging data from multiple studies published between 2000 and 2019 to investigate the differences between adults with addiction and healthy controls during the processing of non-addiction (mainly monetary) gains and losses. By applying criteria that were more stringent than those of the previous meta-analysis, we hoped to provide a better understanding of the nature and direction of impaired neural activity in addiction. Because the differences in loss processing between people with addiction and healthy controls seem to be less well understood, we hoped to gain more insights in this regard. Finally, we hoped to provide indications for future research with the aim of developing interventions for substance dependence and gambling addiction.
Methods
Study selection
We searched Scopus, PubMed and Web of Science for articles published in English from Jan. 1, 2000, to Dec. 1, 2019, using the following terms and their derivatives: “functional magnetic resonance imaging” OR “fMRI”; AND “reward” OR “reward processing”; AND “loss processing”; AND “drug abuse” OR “drug use” OR “drug addiction” OR “substance use” OR “substance dependence” OR “cocaine” OR “marijuana” OR “cannabis” OR “THC” OR “methamphetamine” OR “amphetamine” OR “ecstasy” OR “MDMA” OR “heroin” OR “opiate” OR “opioid addiction” OR “polysubstance” OR “alcohol” OR “cigarette” OR “nicotine dependence” OR “alcohol abuse” OR “alcohol dependence” OR “alcohol addiction” OR “nicotine addiction.” We also examined the reference lists of relevant review articles to include additional papers.
A study was included if it was published in English in a peer-reviewed journal between 2000 and 2019, used fMRI, compared neural activation between adult human participants with substance dependence or gambling addiction and adult human healthy controls, used tasks that required participants to complete an action to obtain rewards and/or avoid losses, and reported significant results of whole-brain analyses as 3-dimensional coordinates in standard stereotactic coordinate space (i.e., Talairach or Montreal Neurological Institute).
A study was excluded if it was conducted in non-human or non-adult participants, did not include a healthy control group, included occasional users (e.g., occasional smokers) in the addiction group and/or the control group, used the same patient data as other included studies, was a diffusion tensor imaging study or a connectivity study, did not examine task-based neural activation (e.g., resting-state fMRI study), involved tasks in which rewarding stimuli or losing events were presented passively, or included only ROI findings. Reviews and meta-analyses were also excluded.
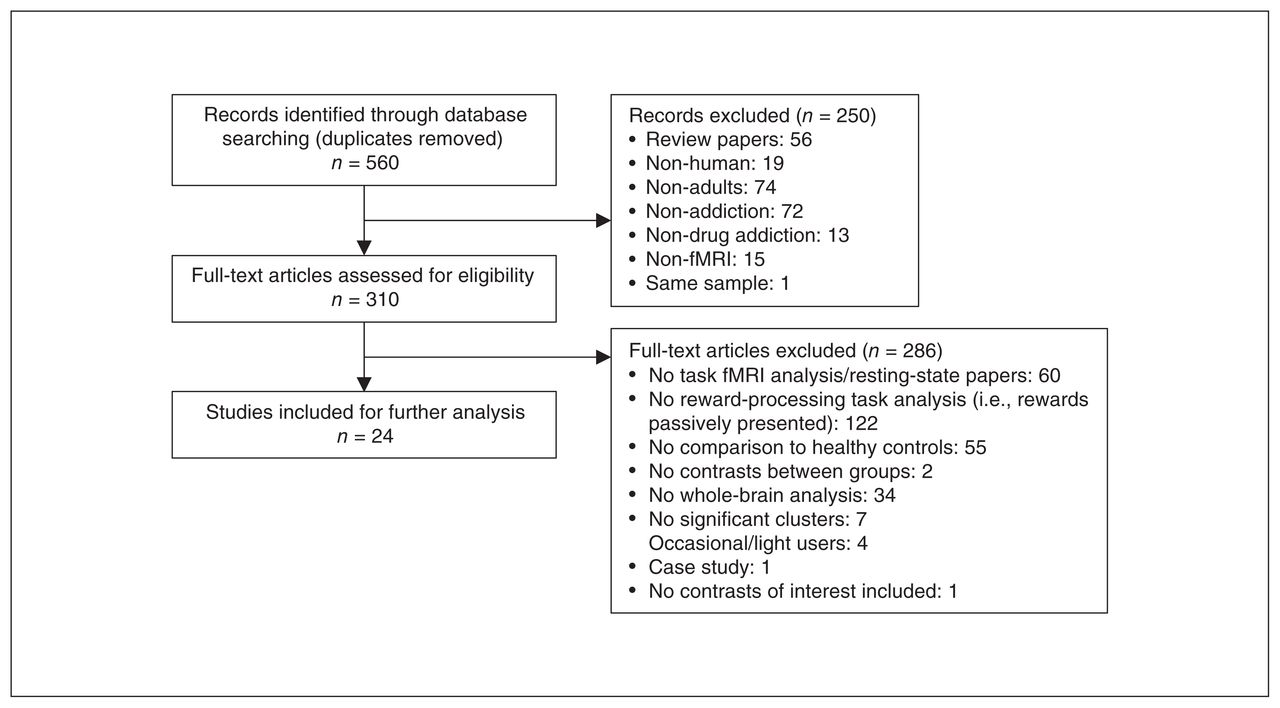
We assessed the quality of each study included in this meta-analysis using a 9-point checklist (Appendix 1, Table S1, available at jpn.ca/200047-a1). The current study was performed according to the Meta-analysis of Observational Studies in Epidemiology guidelines.36 See Figure 1 for the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram indicating the number of studies located and included.
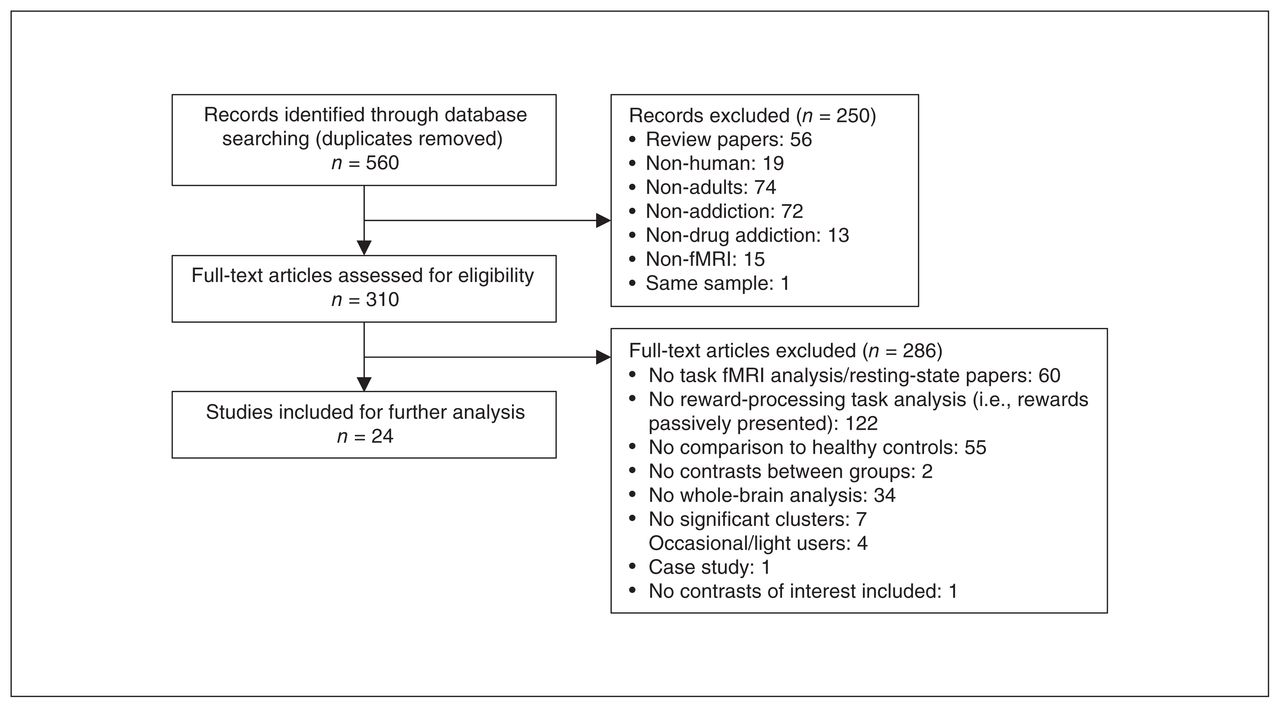
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection. fMRI = functional MRI.
Statistical analysis
Voxel-wise meta-analysis
We used a seed-based d-mapping software package (SDM version 5.15; www.sdmproject.com/software) to perform meta-analyses on neural activity differences between addiction groups and healthy controls. The SDM approach makes it possible to combine statistical parametric maps and reported peak coordinates, described elsewhere.37–39 To summarize, we first extracted peak coordinates and effect sizes (t-values) of neural activity differences between addiction groups and healthy controls from each included study. We converted the effect sizes, reported as z scores or p values, to t values using an online converter (www.sdmproject.com/utilities/?show = Statistics). Second, we recreated a standard Montreal Neurological Institute map of the activation differences by applying an anisotropic Gaussian kernel for each included study. In contrast to isotropic kernels — which may underestimate the effect size of voxels from the same brain area while overestimating the effect size of voxels from other areas — anisotropic kernels can improve the plausibility of the maps by assigning different values to distinct voxels surrounding a peak based on their spatial correlations.39 Third, we applied a random-effects generalized linear model to generate the mean map by fitting the effect size maps into this model. As a result, included studies were weighted differentially based on their sample sizes, between-study heterogeneities and intra-study variances, amplifying the contributions of studies with larger sample sizes or lower variance.38
We conducted meta-analyses between all addiction groups and healthy controls for different combinations of phases of gain and loss processing (i.e., anticipation and outcome) and outcome types (i.e., gain and loss): gain anticipation, loss anticipation and gain outcome. In most studies, the anticipation phase was the waiting period after the onset of a meaningful cue that signalled a potential gain, loss or neutral outcome (e.g., A1 period in Appendix 1, Figure S1). Following this, participants were required to make an active response to a target; however, in 2 studies18,19 the anticipation phase was defined as the waiting period after participants made a response to the target (e.g., A2 period in Appendix 1, Figure S1). The outcome phase is the period immediately after feedback (i.e., winning, losing or neutral) from participants’ earlier response within the same trial (e.g., outcome period in Appendix 1, Figure S1). For our primary analyses, we conducted meta-analyses of gain–neutral contrasts between addiction groups and healthy controls for both the anticipation and outcome phases, and of loss–neutral contrasts for the anticipation phase. By contrasting responses to gains or losses against a neutral condition or a baseline, we could gather less noisy and more cogent evidence for gain- and loss-related neural abnormalities in people with addiction than by directly comparing gain-related with loss-related responses. We calculated differences between addiction groups and healthy controls in each voxel and determined statistical significance using a standard randomization test.40,41 In this meta-analysis, we used the default kernel size and thresholds in SDM (p < 0.005 with peak height Z > 1 and a cluster extent of > 10 voxels) to optimize sensitivity and control false positives.38,42 We did not conduct comparisons for the loss outcome because of the small number of studies.
We repeated separate meta-analyses for the phase-by-type combinations for the substance dependence subgroup, but not for the gambling addiction subgroup, because of a limited number of studies. And because of insufficient data for variables such as mean duration of substance use, we did not conduct meta-regression analyses in this study.
Jackknife sensitivity analysis
We examined the replicability of the findings by conducting a systematic whole-brain, voxel-based jackknife sensitivity analysis. This involved repeating the main statistical analysis but removing 1 study each time, calculating the stability of the findings using the remaining studies.37 A result for the jackknife sensitivity analysis indicated the ratio between the number of study combinations that produced a significant result in 1 specific region and the number of all study combinations. If a brain region remained significant in all or most of the study combinations, we considered the finding to be highly replicable.
Analyses of heterogeneity and publication bias
We performed a heterogeneity analysis using Q statistic maps to investigate unexplained between-study variability in the findings.38 We also performed Egger’s test to look for potential publication bias in these findings by extracting the values of significant peaks of comparison between the addiction groups and healthy controls.42
Supplementary analyses
We conducted supplementary analyses for gain anticipation and gain outcome by including gain–loss contrasts and gain–neutral contrasts. We did not repeat these analyses for loss anticipation because of a limited number of data sets. To reveal whether differences in definitions of the anticipation phase affected our findings, we repeated the analyses for gain and loss anticipation for all addictions after excluding the 2 studies with different definitions of the anticipation phase.18,19 We did not repeat these analyses for the substance dependence subgroup because of the small number of studies. We did not investigate any sex or gender differences in our extracted data, because the included studies did not report results separately for males and females, or report the differences between males and females.
Results
Included studies and sample characteristics
The literature search yielded 560 publications, and after reviewing the titles and abstracts of all studies, we identified 310 fMRI studies for full-text review. Of the 310 studies, 60 were resting-state fMRI studies that did not investigate task-related brain activations; 122 did not employ tasks that required participants to actively complete an action to obtain a reward or avoid a loss; 55 did not include a healthy control group; 34 did not conduct a whole-brain analysis; 7 did not report significant clusters; and 2 did not compare activation differences between the addiction groups and healthy controls. We excluded these studies from the meta-analysis. We also excluded another 4 studies because occasional users or gamblers were part of either the experimental or the control group. We also excluded 1 case study, and 1 study that did not provide data on the contrasts we needed.
Altogether, we identified 24 studies reporting 26 data sets for the current meta-analysis: 21 substance dependence data sets (465 people with substance dependence and 441 matched healthy controls) and 5 gambling addiction data sets (81 people with gambling addiction and 85 matched healthy controls). Of the 5 gambling addiction studies, 3 did not include participants with a gambling addiction who had comorbid substance dependence. One study included participants with gambling addiction and nicotine dependence, but the authors conducted additional analyses controlling for participants’ smoking status and found no confounding effect of smoking habits on the results.43 Another study included participants with both gambling addiction and nicotine dependence and did not investigate the effects of nicotine dependence.21 However, this study did not affect our results because we did not conduct a separate subgroup analysis on gambling addiction. The demographic and clinical characteristics of the included studies are shown in Table 1. The quality score for each study and other information (including experimental paradigms and image acquisition techniques) can be found in Appendix 1, Tables S1 to S3.
Demographic and clinical characteristics of the data set included in the meta-analysis
Gain anticipation
All addictions versus healthy controls
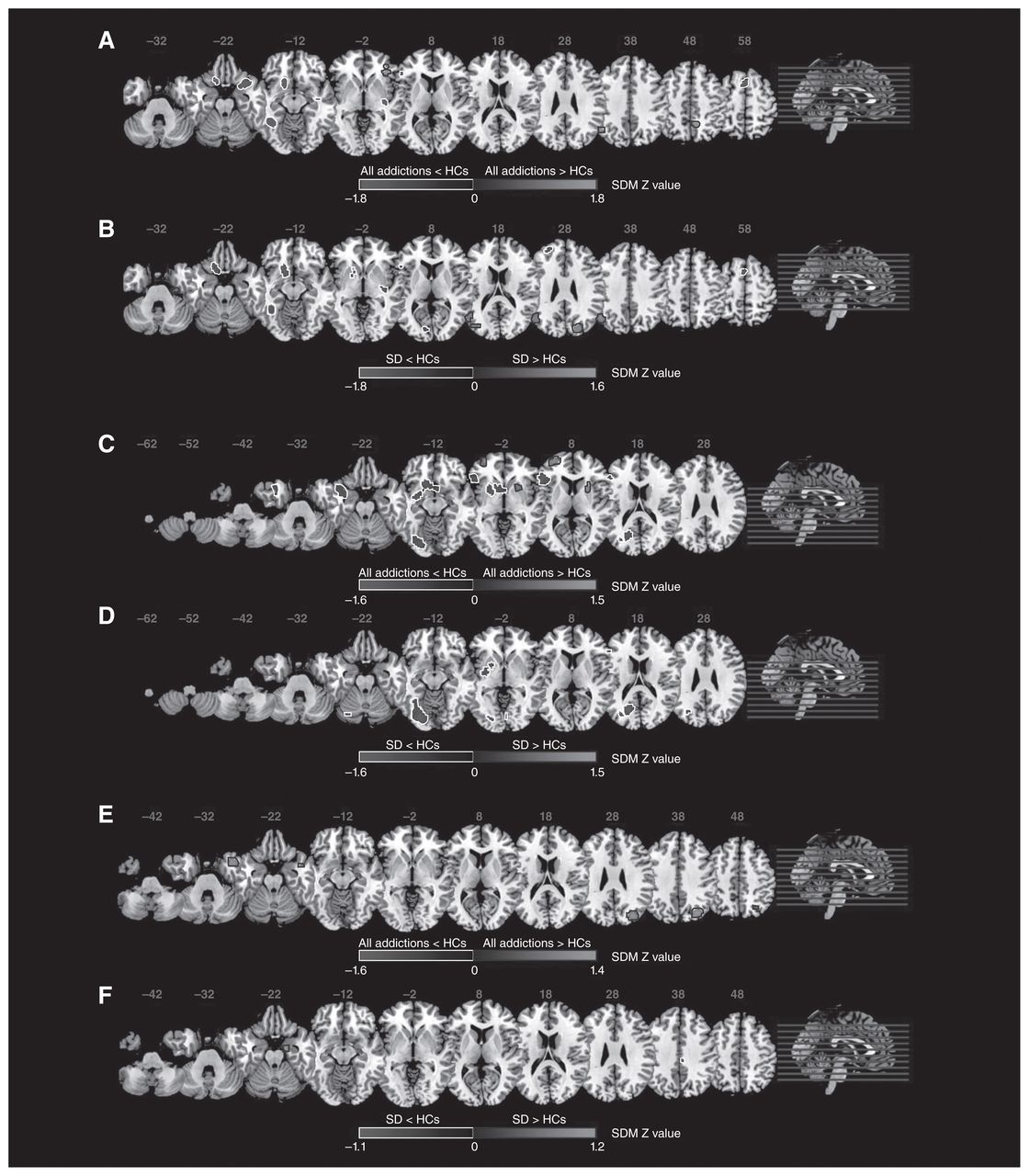
Twelve studies were included in the comparison of all addictions and healthy controls. All addictions exhibited significant hyperactivation in the left angular gyrus/inferior parietal gyrus (extending to the left middle temporal gyrus; Brodmann areas [BAs] 22, 39) and right precuneus. All addictions showed hypoactivation in the left striatum, bilateral inferior frontal gyrus (BAs 11, 38, 45), bilateral supplementary motor areas (BAs 6, 8), left fusiform gyrus (BA 37) and right superior temporal gyrus (extending to the right insula; BA 38). See Figure 2A and Table 2 for detailed results.

Results of the meta-analyses for regional differences of task-evoked activation. (A) All addictions and healthy controls during gain anticipation; (B) the substance dependence subgroup and healthy controls during gain anticipation; (C) all addictions and healthy controls during loss anticipation; (D) the substance dependence subgroup and healthy controls during loss anticipation; (E) all addictions and healthy controls during gain outcome; the substance dependence subgroup and healthy controls during gain outcome. Areas with hypoactivity are outined in white, and areas with hyperactivity are outlined in black. The shaded bars indicate maximum and minimum SDM Z values. HC = healthy control; SD = substance dependence; SDM = seed-based d-mapping.
Meta-analyses of regional differences for task-evoked activation during gain anticipation for participants with addiction and healthy controls
Substance dependence subgroup versus healthy controls
Eight studies were included in the comparison of the substance dependence subgroup and healthy controls. The substance dependence subgroup exhibited significant hyperactivation in the left angular gyrus (extending to the left middle temporal gyrus; BAs 22, 39), right superior occipital gyrus (BA 19) and left middle occipital gyrus (BA 39). It showed hypoactivation in the left striatum (extending to the left inferior frontal gyrus; BA 11), left middle frontal gyrus (BA 46), left fusiform gyrus (BA 37) and left supplementary motor area (BA 6). See Figure 2B and Table 2 for detailed results.
Loss anticipation
All addictions versus healthy controls
Ten studies were included in the comparison of all addictions and healthy controls. All addictions exhibited significant hyperactivation in the bilateral postcentral gyrus (extending to the left inferior parietal gyrus excluding supramarginal and angular; BAs 3, 4, 6), right striatum, left middle frontal gyrus (extending to the left superior frontal gyrus; BA 10) and right inferior frontal gyrus (opercular part, BA 48). All addictions showed hypoactivation in the bilateral striatum (extending to the left temporal pole; BAs 20, 38, 48), left inferior frontal gyrus (BAs 45, 47, 48) and left fusiform gyrus ( extending to the left lingual gyrus; BAs 18, 19). See Figure 2C and Table 3 for detailed results.
Meta-analyses of regional differences for task-evoked activation during loss anticipation for participants with addiction and healthy controls
Substance dependence subgroup versus healthy controls
Seven studies were included in the comparison of the substance dependence subgroup and healthy controls. The substance dependence subgroup exhibited no significant brain hyperactivation. However, it did show hypoactivation in the left striatum, left lingual gyrus (extending to the left fusiform and left inferior occipital gyrus; BAs 18, 19) and left middle occipital gyrus (BA 19). See Figure 2D and Table 3 for detailed results.
Gain outcome
All addictions versus healthy controls
Fifteen studies were included in the comparison of all addictions and healthy controls. All addictions exhibited significant hyperactivation in the right middle occipital gyrus (extending to the right superior occipital gyrus; BAs 7, 19), and the right temporal pole (BAs 20, 38). They showed no significant brain hypoactivation. See Figure 2E and Table 4 for detailed results.
Meta-analyses of regional differences for task-evoked activation during gain outcome for participants with addiction and healthy controls
Substance dependence subgroup versus healthy controls
Eleven studies were included in the comparison of the substance dependence subgroup and healthy controls. The substance dependence subgroup exhibited significant hyperactivation in the right hippocampus (BA 28). It showed hypoactivation in the right median cingulate/paracingulate gyri (BA 23). See Figure 2F and Table 4 for detailed results.
Jackknife sensitivity analysis
The findings described above remained largely unchanged under jackknife sensitivity analysis, indicating high robustness (Tables 2–4).
Analyses of heterogeneity and publication bias
The heterogeneity analysis showed nonsignificant results for most of the reported regions, except the left striatum for the comparisons of all addictions and the substance dependence subgroup versus healthy controls during gain anticipation. The results of the heterogeneity analysis and Egger’s test are summarized in Tables 2–4.
Supplementary analyses
The results of the meta-analyses of gain–loss and gain–neutral contrasts are shown in Appendix 1, Tables S4 (gain anticipation) and S5 (gain outcome). The results from analyses after excluding the 2 studies with a different definition of the anticipation phase are shown in Appendix 1, Tables S6 (gain anticipation) and S7 (loss anticipation).
Discussion
Our results revealed several patterns of altered brain activation for people with addiction during gain and loss processing, providing new evidence of the neural abnormalities in addiction. First, during gain anticipation, all addictions showed reduced brain activation in the striatum, PFC and insula compared to healthy controls, and enhanced brain activation in the precuneus, angular gyrus, middle temporal gyrus and inferior parietal gyrus. The substance dependence subgroup showed very similar patterns, with additional hyperactivation in the occipital lobe. Second, during loss anticipation, all addictions exhibited enhanced activation in the striatum and PFC compared to healthy controls. However, the striatum also showed attenuated activity. A separate analysis for the substance dependence subgroup revealed hypoactivation in the striatum and occipital lobe. Third, during gain outcome, all addictions showed enhanced activation in the occipital lobe.
Neural alterations during gain anticipation
All addictions exhibited decreased activation in the PFC (BA 45, inferior frontal gyrus), left striatum and right insula compared to healthy controls (Fig. 2A and Table 2). The striatum and PFC are important components of the reward network. The striatum is crucial for reward experiences and learning,60 and the PFC is crucial for reward-based decision-making61 and higher-level executive functions, including goal representation and action planning.62,63 Functional interconnections between the PFC and the striatum are responsible for reward detection and regulation.63 Our results were consistent with those of previous reports of reduced PFC and striatal activity in substance detection27 and gambling addiction.22,24,58 These results could be validated by the incentive sensitization theory32,33 and the reward deficiency hypothesis,64,65 both of which predict attenuated activity in the reward system during anticipation of non-addiction-related gains. According to the incentive sensitization theory, the neural system of a person with addiction attributes higher incentive salience to addiction-related rewards (e.g., drugs) and less incentive salience to non-addiction-related rewards (e.g., monetary gains). As a result, non-addiction-related stimuli used in the experiments may be rendered less salient for people with addiction, leading to reduced activation of the reward network (i.e., PFC and striatum). According to the reward deficiency hypothesis, however, hypoactivity in the reward network is an indicator of a deficient reward system that cannot be adequately activated by rewarding stimuli (i.e., both addiction-related rewards and non-addiction-related rewards). This pattern of activity can also be explained by the reward allostasis model.66,67 According to this model, sensitivity to non-addiction-related gains is reduced as a compensatory process to maintain the stability of the reward functions. Given the limited capacity of the reward circuits, non-addiction-related rewards may be allocated weaker hedonic effects, and addiction-related stimuli may take up more resources. Consequently, the reward circuits should be less activated for people with addiction during anticipation of non-addiction-related gains.
We also observed reduced activity in the right insula (Fig. 2A and Table 2). The insula is an important brain region for the integration of internal bodily information, necessary for interoceptive awareness and emotional arousal.68 Previous studies have consistently found decreased insular activity in substance dependence69 and gambling addiction,70 indicating a desensitized interoceptive state. In our study, insular hypoactivation may have denoted weaker interoceptive and emotional responses to non-addiction-related gains compared to addiction-related rewards. In addition, the insula is part of the salience network, which is highly responsive to behaviourally relevant stimuli,71 and was consistently upregulated for people with drug addiction during drug-cue exposure.17 It may be that for people with addiction, addiction-related cues are more relevant than other rewarding stimuli. Compatible with the allostasis model, the attenuated activity of the salience network (i.e., insula) in people with addiction during anticipation of non-addiction-related gains likely functioned as a compensation for its hypersensitivity to addiction-related cues.
In contrast, all addictions showed significantly increased activation in the right precuneus, middle temporal gyrus, inferior parietal gyrus and angular gyrus compared to healthy controls (Fig. 2A and Table 2). These regions are important components of the default mode network, which is responsible for self-referential processing and is normally deactivated during cognitive tasks.72–74 The atypical strengthened activation of the default mode network that we observed in all addictions indicates that the expectation of gains was perhaps associated with the self. It is likely that repeated addictive behaviours in daily life (encompassing the anticipation of the hedonic effects of drugs or monetary wins) are incorporated into self-related memory for people with addiction.75 Therefore, when people with addiction anticipated an imminent reward in the experiments, they were likely prompted by a similar memory of the hedonic sensations. Such an association between gains and self-related memory of hedonic sensations is likely much stronger for people with addiction than for healthy controls,75,76 leading to a stronger activation of the default mode network for people with addiction. In addition, the precuneus is reported to be crucial for the integration of information from our environment.77 It has been suggested that people with addiction showed heightened exteroceptive awareness toward addiction-related cues.77 This result is consistent with cue-elicited hyperactivation in the precuneus in substance dependence,78,79 likely indicating that more salience was assigned to rewarding stimuli, such as drugs. Therefore, non-addiction-related rewards may hold a “bottom–up” attentional advantage for people with addiction compared to healthy controls. Because people with addiction show impaired interoceptive awareness (shown by hypoactivation of the insula) and strengthened exteroception (shown by hyperactivation of the precuneus), it is not surprising that they seem to perform less well when it comes to monitoring their internal feelings and refraining from addictive behaviours.
The results described above were largely the same for the substance dependence subgroup, but they showed additional increased activation of the right superior occipital gyrus and left middle occipital gyrus (Fig. 2B and Table 2). Previous research in rats found that the ability to predict the timing of imminent rewards elicited the activation of the primary visual cortex, which resides in the occipital lobe.80 This finding suggests that gain anticipation can be reflected in very early visual processing in animals. In humans, drug-related visual cues have been associated with increased brain activation in early visual regions for people with substance dependence.81–83 It is likely that for people with drug addiction, frequent and large drug doses increased the responsiveness of the primary visual cortex to cues with rewarding properties. Alterations in the early visual areas are likely specific to substance dependence, because human studies have shown that substance use (i.e., ecstasy) is linked to neurotoxic changes in the occipital lobe84 and heightened excitability of the primary visual cortex.85
Neural alterations during loss anticipation
We found that all addictions showed hyperactivation in the striatum and parts of the PFC (Fig. 2C and Table 3). Several studies have observed hyperactivation in the PFC and striatum in substance dependence and gambling addiction during loss anticipation.19,24,86 It has been argued that increased reactivity to potential losses is associated with salience improperly attributed to imminent losing events,87 which may lead to loss-chasing, a continued behaviour in an attempt to recover losses.1 It has been shown that impulsive behaviours such as loss-chasing are linked to activity in the ventral PFC and striatum.88,89 Specifically, researchers have found that heightened PFC activation in smokers is related to increased craving to relieve smoking abstinence.19 Thus, people with addiction may be more aroused by the forthcoming loss than healthy controls and have the impulse to chase the loss. Loss-chasing is particularly central to gambling addiction.87,90 Thus, the hyperactivities described here may have been driven mainly by the gambling addiction subgroup.
Against this, other researchers have found an opposite trend, which we also observed in the current analysis: decreased striatal activity during loss anticipation in addiction.22,44,58,91 Researchers have suggested that such a hypoactivation is associated with an insensitivity to punishment or loss.91,92 It has been argued that people with addiction are less sensitive to negative consequences (i.e., losses) and may not be able to activate the brain regions responsible for error tracking and adaptive learning.92 The striatum, along with the PFC, is a critical site for these functions,93–96 helping people to learn from negative events and adjust their future behaviours.
The conflicting results described above were perhaps caused by the different natures of gambling addiction and substance dependence, the data for which were included in the analysis of all addictions. The impulse to chase losses is a key symptom of problematic gambling.1 In our analysis of all addictions, hyperactivation of the brain regions linked with impulsive behaviours (i.e., PFC and striatum) may have been driven mainly by the gambling addiction subgroup. Indeed, a separate analysis of substance dependence did not find enhanced brain activity, but the hypoactivation pattern in the striatum remained significant. However, given the limited number of studies we found on gambling addiction during loss anticipation, this explanation remains speculative. Future research should gain more insights into gain and loss processing in gambling addiction.
The substance dependence subgroup showed additional hypoactivation in the left middle occipital gyrus and left inferior occipital gyrus (Fig. 2D and Table 3). Similar to the reward allostasis model,66,67 this pattern can be seen as a compensatory process in which functions of the occipital lobe strive for stability during gain and loss processing. As noted above, the occipital lobe exhibited enhanced activation during gain anticipation for people with drug addiction, possibly indicating increased responsiveness of the primary visual cortex to cues of a rewarding nature (e.g., monetary gains). This change may come at the expense of reactivity to cues of an unrewarding nature (e.g., monetary losses). In other words, it is likely that people with drug addiction allocate few resources to losing events during early visual processing, because the primary visual cortex is more receptive to rewarding stimuli.83 Indeed, the strengthened responsiveness of the visual cortex has been more extensively documented in the literature on gain processing.97 For people with drug addiction to maintain the functional stability of the occipital lobe, loss anticipation should be associated with decreased activation in this region as gain anticipation elicits stronger activation.
Neural alterations during gain outcome
All addictions exhibited increased activity in the right middle occipital gyrus and right superior occipital gyrus (Fig. 2D and Table 4) compared to healthy controls. A previous study found that the occipital lobe was activated more strongly in response to visually presented pleasant stimuli compared to neutral stimuli.98 It was argued that the visual cortex is responsive to affective information from the stimuli we see. In addition, addictive behaviours have been positively associated with neuroticism and extroversion,99–102 2 personality traits that are closely linked to affective sensitivity.103 Therefore, it is conceivable that people with addiction are more responsive than healthy controls are to the emotional components of gain outcomes (i.e., pleasantness), even during early visual processing. Our results supported this by showing hyperactivity in the occipital lobe in response to rewarding outcomes.
We observed no significant hyper- or hypoactivation of the PFC or striatum during gain outcome. This was not surprising, because several studies have obtained similar results.21,51,104 However, the existing literature also provided a large body of evidence showing altered activity in these regions in addiction. For example, some researchers found reduced activation of the PFC in people with addiction during the delivery of gain outcomes.19,22,23,52,56 Others found strengthened activation in both the PFC and striatum.46,48,53 The discrepancies among the different studies may have been due to methodological factors (including task designs) and participant characteristics (such as addiction severity and abstinence stage). For example, although most studies used the monetary incentive delay task105 or a modified version (i.e., substance-unrelated activity incentive delay tasks), some studies used less common paradigms, including the reward prediction task19 and the probabilistic reversal learning task.23 Participants cannot control the outcomes in paradigms such as the reward prediction task, but they can obtain monetary gains or avoid losses in a monetary incentive delay task.22,24 It may be that the responses to predetermined outcomes and the responses to rewards that were actively obtained induced different activation patterns in the brain. In addition, the length of abstinence has been negatively associated with brain activity in monetary gain.106 Differences in participants’ abstinence stages or treatment-seeking status were likely other important factors contributing to the conflicting results.
It is also worth mentioning that the absence of elevated striatal activity during gain outcome in our study was inconsistent with the meta-analysis by Luijten and colleagues.27 This was perhaps because our study selection criteria differed from their work in 2 main aspects. First, we included studies comparing gain- or loss-related responses to responses in neutral conditions (i.e., no-win or no-gain) or a baseline, whereas Luijten and colleagues also included gain–loss contrasts. Second, we included data from whole-brain analyses only, whereas they also used data from ROI analyses. As a result, only half of the studies included in our work overlapped with theirs. In addition, because our meta-analysis was conducted more recently, there were more substance dependence data sets (i.e., 21) than in the previous meta-analysis (i.e., 15).
Loss anticipation versus gain anticipation
Previous meta-analyses or reviews did not provide systematic or conclusive findings on loss processing in addiction,27,107 possibly because some researchers did not include or report on loss-related trials.106,108,109 In this study, we compared alterations in brain activity during loss anticipation to gain anticipation in people with addiction.
First, although loss anticipation activated the PFC and striatum, gain anticipation showed no such hyperactivity. This was perhaps because the impulse to chase losses was present only when there was the possibility of losing, leading to enhanced activity in regions associated with impulsivity (i.e., the PFC and striatum). Second, we observed enhanced activation in several posterior parietal areas (e.g., the precuneus and angular gyrus) during anticipation for gains but not losses. The posterior parietal lobe is an important site for spatial awareness and attention.110 It is likely that forthcoming rewards in the environments hold a “bottom–up” attentional advantage for people with addiction, who tend to intentionally seek pleasure through taking drugs or gambling. But such activities were not present when they anticipated a losing outcome. This finding seems to suggest that people with addiction allocate more attentional resources to gains than losses.
Furthermore, we observed hypoactivity in the PFC and striatum during both gain and loss anticipation. This was inconsistent with the previous literature, which found robust ventral striatal activities in expectation of both positive and negative outcomes.111–113 Diminished activity in the reward circuits may indicate impaired reward value updating and adaptive learning.93,95,114 People with addiction may have difficulty updating the subjective reward value of the substance and consequently require more of the substance to obtain pleasurable effects. This is likely one of the reasons why people with addiction tend to increase drug dosage or administration frequencies over time.115 Although we interpreted the hypoactivity during gain anticipation as a result of sensitization processes, we proposed that the striatal hypoactivation during loss anticipation was due to insensitivity to losses in people with addiction. Alternatively, we offer a parsimonious explanation for these results altogether by applying the reward allostasis model again.66,67 According to this model, the attenuation of the PFC and striatum is likely a compensatory process for people with addiction to maintain the stability of the reward function. That is, people with addiction allocate more resources from the reward network to addiction-related cues at the expense of its reactivity to non-addiction-related gains and losses. By the same token, in areas involved in early visual processing (i.e., the occipital lobe), activity was strengthened during gain anticipation but attenuated during loss anticipation for people with drug addiction. It is possible that the reduced reactivity of the occipital lobe to anticipatory losses was a compensatory process to reach functional stability of the primary visual cortex.
Conditioning perspective
It is worth noting that some of our findings can be explained by the conditioning literature. The experimental tasks used in the included studies (especially monetary incentive delay tasks) encompassed components of both classical conditioning and operant conditioning.116 Specifically, a cue that predicted a potential gain or loss can be seen as a conditioned stimulus, while a delivered outcome can be considered an unconditioned stimulus, forming classical conditioning.29 Participants’ action during the anticipation phase can then be considered a conditioned response, because it was preceded or triggered by a cue. In the meantime, because the specific value of an outcome (i.e., win $1 or win $0) was contingent on participants’ actions, the response–outcome association formed an operant conditioning in which the outcome could also reinforce participants to adapt their actions to maximize gains and minimize losses. Therefore, it is reasonable to expect brain activity in regions related to both types of conditioning during these gain and loss processing tasks. Indeed, we found lower activation of the striatum during the anticipation phase in people with addiction compared to healthy controls. Previous research has found that the striatum is crucial in human classical and operant conditioning.117,118 Hypoactivity in this region may indicate impaired associative learning,119 especially punishment-based (e.g., monetary loss) learning,120 in people with addiction. As pointed out earlier, the components of classical and operant conditioning are intricately entangled in gain and loss processing paradigms: the cue-outcome association forms a classical conditioning, and the response-outcome association forms an operant conditioning. Moreover, because we contrasted gain and loss responses against a neutral condition or baseline, the effect of conditioning may have been weakened in the extracted data. Consequently, the majority of our findings may not be entirely interpretable under the conditioning framework. Future research can aim at gaining further insights into conditioning in people with addiction by applying established conditioning paradigms.
Limitations
There were some limitations in this study. First, the number of included studies on gambling addiction was very small. Because of relatively stringent inclusion criteria, we identified and included only 5 studies on gambling addiction. Thus, we were unable to investigate unique alterations in the brain for people with gambling addiction from the perspective of a meta-analysis. Such a limitation kept us from making conclusive statements about some of the brain activation patterns we observed. For example, was the hyperactivity in the PFC and striatum during loss anticipation indeed driven by the gambling addiction subgroup? Is there any increased activation in the occipital lobe for people with gambling addiction during gain anticipation? Second, only a few studies included in our meta-analysis reported clinical information about the participants (i.e., mean duration of substance use and age of onset of use). As a result, we were unable to conduct regression analysis, which could have revealed if there were any moderating effects of clinical traits on the neural abnormalities. Future research should gain more insight into the altered brain mechanisms in gambling addiction and emphasize the clinical attributes of the patients. Third, some included studies24,47,50,51 controlled for potential confounding variables in their analyses and reported adjusted effect sizes for the peak coordinates (e.g., t values), but the majority of studies did not control for variables of no interest and reported unadjusted statistics. This inconsistency in controlling for confounders and reporting related effect sizes may have had some influence on our findings, but we infer that the effect(s) should be relatively minor because almost all included studies discounted the possibility of potential confounders driving the results by, for instance, matching the participants in advance or conducting correlational analyses between the findings and confounders post hoc. Finally, we included only studies in adults with addiction in our analyses. This was because non-adults, especially adolescents, undergo significant structural and functional changes in reward-related brain regions that are not fully developed until their mid-20s.121 It is not yet clear how these changes may influence adolescents’ susceptibility to addictive behaviours.122 Moreover, although many adolescents try drugs, only a small group of them transition to substance dependence.123 On these grounds, we investigated only adults with addiction.
Conclusion
This meta-analysis revealed several brain regions that showed altered activity during gain and loss processing in adults with addiction. Compared to healthy controls, all addictions showed attenuated activity in the PFC, striatum and insula and enhanced activity in several regions in the default mode network (e.g., the precuneus and angular gyrus) during gain anticipation; enhanced activity in the PFC and conflicting results regarding the striatum (which showed both hyper- and hypoactivation) during loss anticipation; and enhanced activity in the occipital lobe during gain outcome. For the substance dependence subgroup, activity in the occipital lobe was strengthened during gain anticipation but attenuated during loss anticipation. We identified altered brain activity for people with addiction not only in the reward network, but also in regions across the brain, some associated with higher-level functions (i.e., salience network and default mode network) and others associated with lower-level functions (i.e., the primary visual cortex). We also found that people with addiction seemed to be more aroused by and more sensitive to forthcoming gains than losses, demonstrated at both higher-level brain regions (i.e., posterior parietal lobe) and lower-level areas (i.e., the primary visual cortex). Finally and most importantly, we used an allostasis model to explain most of the brain activation patterns in terms of the functional stability of the relevant regions: the reward and salience networks for addiction-related stimuli versus non-addiction-related stimuli, and the occipital lobe for gains versus losses. These results may help us to understand the pathology of gain and loss processing in addiction.
Footnotes
Competing interests: No competing interests declared.
Contributors: Z. Qiu and J. Wang designed the study. Z. Qiu acquired the data, which both authors analyzed. Both authors wrote the article, which both authors reviewed. Both authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
Funding: This study was funded by the National Natural Science Foundation of China (81801685); National Natural Science Foundation of Guangdong Province, China (2018A030310003).
- Received March 9, 2020.
- Revision received July 8, 2020.
- Accepted July 10, 2020.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is non-commercial (i.e. research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.