

Abstract
Background Reconsolidation impairment using propranolol is a novel intervention for mental disorders with an emotional memory at their core. In this systematic review and meta-analysis, we examined the evidence for this intervention in healthy and clinical adult samples.
Methods We searched 8 databases for randomized, double-blind studies that involved at least 1 propranolol group and 1 placebo group. We conducted a meta-analysis of 14 studies (n = 478) in healthy adults and 12 studies in clinical samples (n = 446).
Results Compared to placebo, reconsolidation impairment under propranolol resulted in reduced recall of aversive material and cue-elicited conditioned emotional responses in healthy adults, as evidenced by an effect size (Hedges g) of −0.51 (p = 0.002, 2-tailed). Moreover, compared to placebo, reconsolidation impairment under propranolol alleviated psychiatric symptoms and reduced cue-elicited reactivity in clinical samples with posttraumatic stress disorder, addiction or phobia (g = −0.42, p = 0.010).
Limitations Methodological differences between studies posed an obstacle for identifying sources of heterogeneity.
Conclusion Reconsolidation impairment is a robust, well-replicated phenomenon in humans. Its clinical use is promising and deserves further controlled investigation.
Introduction
Increased activation of the stress response during emotional experiences plays the adaptive role of enhancing memory consolidation and facilitating subsequent recall.1–3 Preclinical evidence suggests that the consolidation of both aversive and appetitive memories is dependent on the activation of the noradrenergic system in the basolateral amygdala. Heightened activity in these mechanisms may lead to an overly powerful emotional memory thought to underlie certain psychiatric disorders.3,4 For instance, it is thought that exposure to highly stressful or traumatic experiences that accentuate the stress response may underlie aversive memories in fear-based psychiatric disorders, such as posttraumatic stress disorder (PTSD), adjustment disorder and specific phobia, among others.2,5 As well, overly consolidated appetitive memories of drug-use experiences arguably maintain compulsive drug-seeking behaviours in people with addiction.6 More precisely, overly consolidated memories become too easily reactivated, perpetuating symptoms of intrusion, avoidance and hypervigilance in trauma- and stressor-related disorders and phobias,2,7 and craving and relapse in substance dependence.8 Considering the role of emotional memories in such disorders, reducing the strength of these memories would have obvious clinical value and deserves to be attempted.
Memory reconsolidation theory suggests the presence of a neuroplastic process whereby the reactivation of previously consolidated memories induces a temporary state of lability, during which time such memories may be altered before restabilizing.9 It is argued that this mechanism may be implicated in updating or impairing long-term memories by interfering with their restabilization back to long-term storage (i.e., reconsolidation). As with initial consolidation, reconsolidation is also dependent on de novo protein synthesis and activation of the noradrenergic system.10,11 Evidence suggests that propranolol — a synthetic noradrenergic β-receptor blocker that crosses the blood–brain barrier and exerts central inhibitory effects — can oppose the enhancement of memory conferred by emotion when administered before or shortly after new learning (consolidation) or the recall of established memories (reconsolidation).12–14 Although the mechanisms of reconsolidation require clarification, one possibility is that by blocking noradrenergic activity in the amygdala, propranolol disrupts the cyclic AMP/protein kinase A pathway, indirectly interfering with the synthesis of new proteins required for memory (re)consolidation.15–17
Therapeutic approaches based on reconsolidation interference theory offer hope for a paradigm shift in the treatment of mental disorders that have an emotional memory at their core.18–22 A previous meta-analysis of studies of experimentally acquired and previously learned emotional memories demonstrated that the reconsolidation blocker propranolol, paired with memory reactivation, weakened such memories compared to memory reactivation under placebo in healthy adults.14
Based on such findings, reconsolidation impairment procedures are being adapted increasingly into treatment protocols for several psychiatric conditions. For instance, one protocol involves reactivating a traumatic memory by writing a narrative and reading it aloud after the administration of propranolol. This protocol has shown efficacy in improving both trauma- and stressor-related and substance-dependence symptoms.23,24 Similar protocols that elicit memory retrieval (reactivation) using videos, words or in vivo exposure to substance cues or fearful stimuli have also shown efficacy.7,25,26 However, some studies have failed to find such effects.27,28 One meta-analysis examined the reconsolidation of naturalistic memories in clinical and subclinical samples; although the authors reported promising results, they concluded that heterogeneity among studies limited the strength of the findings.29
An up-to-date review and meta-analysis of randomized controlled trials that have examined the impairment of emotional memory reconsolidation using propranolol in healthy and clinical samples may help to further explore this issue. We hypothesized that, compared to placebo, memory reactivation under the influence of or followed by the reconsolidation blocker propranolol would reduce recall, recognition memory and psychophysiological responding, and that it would decrease symptom severity in clinical samples.
Methods
Study inclusion criteria
We included studies in the qualitative synthesis if they were published (with no date constraint) and involved memory reactivation under propranolol in human adults. We included studies in the meta-analysis if they met the criteria above and were double-blind, placebo-controlled trials.
Experimental paradigms
The protocols typically used in reconsolidation studies that involve healthy volunteers consist of behavioural learning (e.g., conditioned responses to emotional material), physiologic reactivity to autobiographical emotional memories using script-driven imagery (i.e., symptom provocation) or declarative memory tasks. Protocols typically involve 3 phases: (1) participants undergo initial learning of emotionally valenced or neutral material (e.g., word lists, pictures or conditioned stimuli); (2) at least 24 hours later, propranolol or placebo is administered 60–90 minutes before or immediately after memory reactivation achieved by the brief presentation of a cue; and (3) after a washout period of 24 hours, participants’ memory is tested via a recall or recognition task, or via physiologic reactivity to the conditioned stimulus.
In single-treatment clinical studies, memory reactivation is achieved by exposing participants to salient fear- or drug-related cues before or after the administration of propranolol (or placebo), and declarative memory or physiologic reactivity is tested after a washout period of at least 24 hours. In other clinical studies, the typical treatment protocol involves drug administration 60–90 minutes before participants are asked to write and read aloud a 1-page narrative of the traumatic experience over multiple6 treatment sessions, after which symptom severity or physiologic reactivity is measured.23,30
Outcome measures
For healthy samples, the outcome of interest for studies involving declarative memory tasks was memory performance for emotional material on the test day, as measured by free recall or percent correct on a recognition task. The outcome of interest for studies involving conditioned responses to emotional material consisted of physiologic responses. For clinical samples, the primary outcomes of interest were symptom severity as measured by self-report or clinician-rated measures, physiologic responding to symptom provocation (i.e., heart rate, skin conductance or electromyogram), or both.
Search strategy and data extraction
We searched PsycINFO, Ovid Medline, PTSDpubs, Web of Science, Google Scholar, PubMed, Cochrane Central and clinicaltrials.org up to September 2021, to find relevant studies using various combinations of the following key words: propranolol, reconsolidation, reactivation, emotion*, memory, fear, reward, trauma, anxiety, post-traumatic, post-traumatic stress disorder, PTSD, acute stress disorder, adjustment disorder, phobia, specific phobia, spider phobia, addict*, substance abuse and substance dependence. We exported the results of this search to a reference-management database and removed duplicates.
Three investigators (S.P., O.R. and a research assistant) independently screened the titles and abstracts, excluding irrelevant articles and assessing all relevant full-text articles. The investigators met to compare results, and disagreements were resolved by consensus. We also screened the reference sections of included articles for other articles. We conducted separate searches and analyses for the healthy and clinical samples. Finally, we contacted researchers in the field to determine whether they had unpublished data that could be included in the meta-analysis.
Data from the included studies were extracted by 3 independent raters (S.P., O.R. and a research assistant) and double-checked by a fourth party (M.L.). When studies reported incomplete results, we contacted the authors. If the authors could not provide the missing data, we excluded the study. Then, 2 research assistants used the Jadad Scale31 to conduct a quality assessment of the included studies.
Statistical analyses
To examine between-group mean differences on the test day (healthy volunteers) or post-treatment (clinical samples), we used Hedges g, because it produces an adjusted effect-size estimate for small samples.32,33 Hedges g is interpreted similarly to Cohen d: g < 0.2 represents a small effect size, 0.2 to 0.5 represents a moderate effect size and 0.6 to 0.8 represents a large effect size.32,33 For studies that reported several outcomes of interest, we averaged Hedges g across outcomes to control for outcome selection bias. Tests of the pooled Hedges g estimate were 2-sided (α < 0.05), which provided a more conservative test of the overall pooled effect. Owing to methodological heterogeneity among studies, we used a random-effects model to test the hypotheses.34 In contrast to a fixed-effects model (which assumes that each included study represents only one “true” effect), a random-effects model assumes that there is a distribution of “true” effects that varies between studies as a function of study characteristics.34 We also conducted homogeneity analyses using Q and I2 statistics to identify outliers and sources of heterogeneity.34,35
We assessed publication bias by visual inspection of funnel plot symmetry; asymmetry indicated possible publication bias. In addition, we used the trim and fill method36 to examine the impact of potential publication bias on the pooled effect size estimate. Finally, we used the Egger test to evaluate the presence of bias reflected in the funnel plot (a 2-tailed p-value < 0.05 indicated significant bias).34,36 We performed analyses using Comprehensive Meta-Analysis software (version 3; Biostat Inc.).
Results
Figure 1 displays the PRISMA flow diagram for study selection. Across 31 publications (36 studies) included in the qualitative synthesis (see qualitative results), 17 studies involved healthy samples,37–51 and 19 involved clinical samples.7,23–28,30,52–59

We excluded 5 clinical studies from the meta-analysis because they did not include a placebo group.30,55,57 We excluded 3 studies involving healthy samples49,51 and 2 involving clinical samples25,59 from the meta-analysis because they did not report data in a usable format, and the raw data could not be retrieved from the authors. Moreover, 1 study58 provided between-group effect sizes for the sample at 3 months post-treatment based on the PTSD status of participants at study entry (i.e., moderate PTSD symptoms and severe PTSD symptoms). We included these as such in the meta-analysis. Thus, across 24 publications, 26 studies were included in the meta-analysis: 14 involving healthy samples37–48,50 and 12 involving clinical samples.7,23,24,26–28,52–54,56,58
Qualitative results
Table 1 summarizes the characteristics of the studies included in the qualitative synthesis, but not in the meta-analysis. Table 2 and Table 3 summarize the characteristics of the healthy adult and clinical studies, respectively, that were included in the quantitative synthesis. Across all studies, 618 participants received propranolol and 527 participants received placebo.
Characteristics of studies included in the qualitative review but excluded from the meta-analysis
Characteristics of included reconsolidation interference studies — healthy samples
Characteristics of included reconsolidation interference studies — clinical samples
Studies involving healthy participants
In 11 of the 17 studies involving healthy participants, a differential fear-conditioning paradigm was used. Of these, 8 found that propranolol administered during memory reactivation lowered physiologic responses to fear-conditioned stimuli compared to placebo.40,43,44,46,49–51 In one of these studies, the effect was observed only among participants who expected to receive the unconditioned stimulus during the reactivation trial on day 2 (i.e., the shock), but did not (i.e., prediction error).50 In another study, the between-group effect of propranolol was also observed for when the unconditioned stimulus was the reactivation cue.51
The other 6 studies employed standard emotional material (i.e., a video, a slide show or pictures) or asked participants to write a personal narrative detailing a negative event as the memory task. Of the 6 studies, 4 found that participants who received propranolol remembered less emotional material than those who received a placebo.39,41,42,45
Studies involving clinical samples
Of the 19 studies involving a clinical sample, 8 involved participants with chronic PTSD,23,30,52,55–57 2 involved participants with chronic PTSD comorbid with symptoms of major depression,58 7 involved participants with substance dependence24–28,53,59 and 2 involved participants with specific phobias.7,54
Ten clinical studies used a single reactivation session7,25–28,52–54,57,59 and 9 used several (4–6) sessions.23,24,30,55,56,58 To reactivate the aversive or appetitive memories, 13 studies used written or audiorecorded trauma or drug-use narratives,23,24,27,28,30,52,55–58 4 used other exposure-based or stress-inducing tasks (e.g., public speaking)7,25,53,54 and 2 employed cues from a previously learned list of drug-related words or smoking-related pictures.26,59
Of the 13 studies that used written or auditory trauma or drug-use narratives, 8 found that propranolol-treated participants showed improvements in trauma-related or substance-dependence symptoms.23,24,30,52,55,56 In 1 publication,58 no treatment effect was found for participants with moderate PTSD symptoms at 3 months post-treatment; however, a significant effect was observed for participants with severe PTSD symptoms. Three other studies failed to find an effect of reconsolidation impairment with propranolol compared to placebo.27,28,57 Finally, for 5 of the 6 clinical studies that implemented other exposure-based methods and the studies that used a word list or pictures, propranolol paired with reactivation improved clinical symptoms compared to placebo paired with reactivation at the post-treatment test phase.7,25,26,53,59 The remaining study did not find an effect for propranolol.54
Quantitative results
Quality assessment of studies in the meta-analysis
Of the 26 total studies included in the meta-analysis, 18 had a Jadad score of 3.5 or higher, indicating good methodological quality. To maximize the sample size, we retained studies with lower methodological quality in the meta-analysis and examined study quality as a moderator variable. See Tables 1 and 2 for individual quality assessment ratings.
Studies involving healthy participants
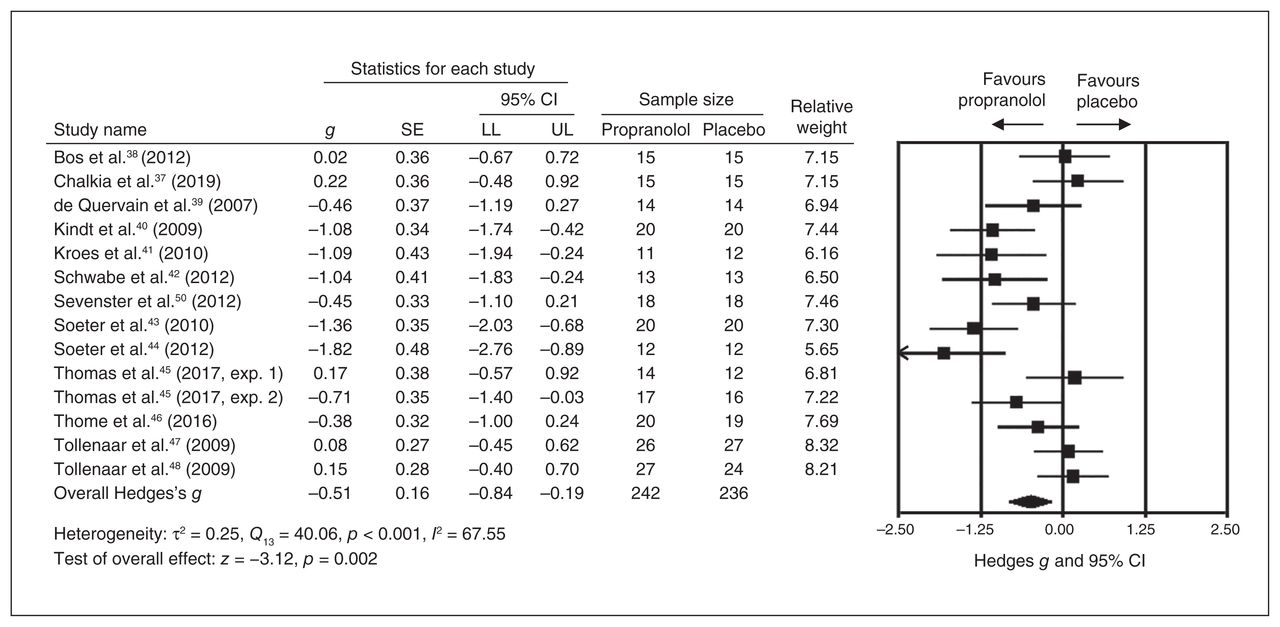
As shown in Figure 2, propranolol-treated participants (n = 242) remembered less aversive material than placebo-treated participants (n = 236; g = −0.51, 95 % CI −0.84 to −0.19; p = 0.002). However, statistical heterogeneity was significant (Q13 = 40.06, p < 0.001; I2 = 67.55 %). Sensitivity analyses revealed no outliers. Effect sizes varied between −1.82 and 0.22.
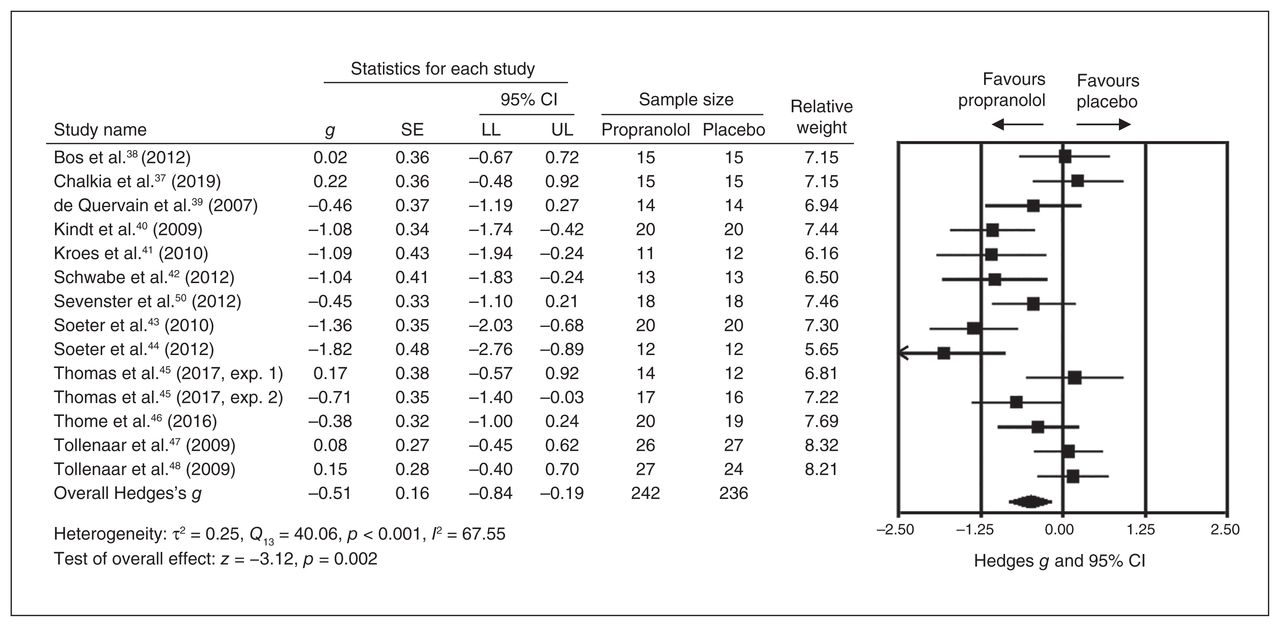
Reconsolidation interference in healthy samples. CI = confidence interval; LL = lower limit; UL = upper limit; SE = standard error.
Studies involving clinical samples
As shown in Figure 3, 236 participants received propranolol and 210 participants received placebo. The studies were heterogeneous (Q11 = 29.96, p = 0.002; I2 = 63.28 %).

Reconsolidation interference in clinical samples. CI = confidence interval; LL = lower limit; UL = upper limit; SE = standard error.
Memory reactivation under propranolol reduced symptom severity and cue-induced physiologic reactivity compared to memory reactivation under placebo, with a moderate to strong effect size in 7 of 12 studies (g = −1.28 to −0.51).7,23,26,52,53,56,58 The overall effect size was moderate, and the difference was significant in favour of propranolol (g = −0.42, 95 % CI −0.74 to −0.10; p = 0.010). Effect sizes ranged between −1.28 and 0.60. According to sensitivity analyses, no single study explained the heterogeneity we observed.
Publication bias
Analysis of publication bias in the healthy samples revealed a relatively symmetrical funnel plot, and results from the trim and fill analysis under a random-effects model indicated that no studies to the right of the mean (i.e., null or negative findings) were missing from the funnel plot. However, the result of the Egger test was statistically significant (p = 0.023), suggesting a risk of publication bias (i.e., small studies reporting large effects).
Concerning the clinical samples, analyses revealed a relatively symmetric funnel plot, and results from the trim and fill analysis under a random-effects model indicated that no studies to the right of the mean were missing from the funnel plot. The result of the Egger test was not statistically significant (p = 0.31), suggesting little risk of publication bias.
Exploring sources of heterogeneity
We conducted post hoc analyses to explore whether moderating variables explained the heterogeneity we observed. Specifically, we examined the following variables separately in both healthy and clinical samples: outcome measured (i.e., declarative memory v. physiologic reactivity in healthy samples; symptom severity v. physiologic reactivity in clinical samples); medication dosage (40 mg v. other dosages); medication timing (pre-reactivation v. post-reactivation); sex (male v. female); and study quality (good v. poor). We used the delay before the memory test or symptom measurement (1 d v. 1 wk) as a moderator for analysis of only the healthy samples because a limited number of clinical studies measured outcomes after 1 day. None of these variables explained the observed heterogeneity.
Finally, for clinical samples only, we examined whether memory valence (aversive v. appetitive) moderated the strength of the effect size. The overall effect size was larger for studies that involved aversive memories (e.g., trauma or phobia; g = −0.53, p = 0.016) than for those involving appetitive memories (e.g., drug-related; g = −0.27, p = 0.29), although the between-group difference was not statistically significant (Q1 = 0.587, p = 0.44).
Discussion
Emotional memories can be successfully weakened by administration of the reconsolidation blocker propranolol paired with memory reactivation. Cue-induced physiologic reactivity and declarative memory for emotional material was reduced in healthy individuals who reactivated a memory under propranolol compared to those who did it under placebo. This finding was consistent with the findings of the meta-analysis by Lonergan and colleagues14 and was congruent with reconsolidation interference theory.
In clinical samples, reactivating a pathogenic memory under propranolol reduced symptom severity and related physiologic reactivity in participants with PTSD, specific phobia or substance dependence, using a personal trauma or drug-use narrative or other exposure-based methods. Arguably (and similar to studies involving healthy samples in fearconditioning or cue-induced reactivity paradigms), a reduction in physiologic responding to traumatic, phobic or drug-using memory can be considered an indicator of a change in the memory (e.g., reduced salience), such that the memory is less capable of symptom provocation.60 This finding was also congruent with reconsolidation interference theory and supported the clinical efficacy of this intervention. Importantly, the strength of the effect size in clinical samples was in line with the efficacy of established psychotherapies for the same disorders, such as cognitive behavioural therapy for PTSD.61,62 In addition, of the 7 clinical studies that were excluded from meta-analysis, 530,55,59 found a treatment effect in favour of propranolol, suggesting that incorporating these studies into a meta-analysis may have increased the overall effect.
One study of participants with PTSD and comorbid depression58 did not find an effect of propranolol that surpassed their placebo group at 1 week post-treatment; however, a treatment effect was observed among participants with severe PTSD and at 3 months post-treatment. It is possible that for severe cases of PTSD, reconsolidation impairment with propranolol may be efficacious in the longer term, considering that, unlike other exposure-based therapies, reconsolidation is unlikely to be prone to relapse. However, there was no mention in this study of a protocolized treatment manual or treatment adherence monitoring and rating. Thus, the influence of such factors on the observed effect could not be assessed.
Contrary to our previous meta-analysis,14 the current results for reconsolidation impairment in healthy samples showed no moderation effect for medication dosage (40 mg v. 80 mg), delay between drug administration and recall (24 h v. 1 wk) or participant sex. Considering that the moderation observed in the earlier meta-analysis was driven by 2 studies, it seems that increasing the number of included studies watered down the observed effects. Moreover, the results of the meta-analysis of studies in clinical samples did not reveal significant moderation by any sample characteristic (e.g., sex, type of psychological disorder) or methodological difference (e.g., type of outcome measured, medication dosage, medication timing, delay before memory test or symptom measurement).
Although methodological differences did not moderate the findings in either analysis, a great deal of variation existed across the examined studies that was related mainly to the memory-reactivation procedures (i.e., stimuli used, drug dosage or timing, number of sessions). This variability complicated our ability to contrast studies and identify the ideal protocol for conducting reconsolidation impairment. Although the included studies were deemed sufficiently homogeneous to provide a meaningful synthesis under a random-effects model,34,63 one issue may have been related to the type of disorder under study. In this analysis, fear-based (i.e., trauma or phobia) studies demonstrated a larger overall effect than drug-related studies. Although this may have been related to nuances in the neurobiological substrates involved in drug-related learning,8,28 it may also have been because of methodological factors within studies (i.e., the duration of the reactivation session; see also Walsh and colleagues29). Thus, establishment of a standardized treatment protocol that can be implemented in research settings is desirable to identify variables related to treatment efficacy.
One last factor that may have contributed to the observed heterogeneity was the notion of mismatch or prediction error.64 For memories to enter a state of lability, new or unexpected information must be provided.50,65 Without this mismatch, the memory would not destabilize, and retrieval would not set the stage for reconsolidation, thus preventing propranolol from playing its role of reconsolidation impairment. Therefore, it may be necessary for mismatch to be integrated into the memory-reactivation procedures to improve the validity and efficacy of reconsolidation impairment as a psychiatric treatment.66 Of the studies included in this analysis, only one intentionally incorporated prediction error into a study involving healthy volunteers.50 The absence of mismatch in some reconsolidation studies, particularly in clinical samples, may explain some of the negative findings.67–69
Limitations
As discussed, the relatively small number of included studies, and the methodological differences between them, precluded an in-depth assessment of potential moderators of between-group effects of reconsolidation impairment using propranolol. In line with this, reporting biases within and between included studies may have not only contributed to the observed heterogeneity, but also introduced bias in the effect-size estimates. We specifically chose Hedges g for this analysis because it corrects for overestimation of between-group effects associated with small samples, and because we wanted to maintain consistency with previously published meta-analyses.14,29 However, Hedges g performs best under parametric assumptions in the source studies. Future meta-analyses may opt to explore nonparametric measures of effect size (e.g., probability of superiority) to further expand on our findings.70
Conclusion
Findings from this meta-analysis suggest that compared to placebo, propranolol paired with memory reactivation can weaken emotional memories in healthy participants and clinical samples. The findings of this meta-analysis highlight the need to identify the essential procedural components required to successfully induce and impair memory reconsolidation in clinical samples to maximize treatment efficacy. Clarifying the ideal method for impairing reconsolidation would extend our understanding of the mechanisms through which memory reconsolidation occurs and help shed light on how to consistently ensure better treatment outcomes. Furthermore, future studies should test how to systematically incorporate mismatch into reconsolidation impairment, and whether this improves outcome.
The current findings bridge an important gap between pre-clinical experimental findings and the clinical implementation of reconsolidation impairment. Reconsolidation impairment using propranolol is an innovative intervention with far-reaching clinical implications in the field of psychiatry, considering that a number of mental disorders stem from pathological memories.
Acknowledgements
The authors wish to thank Reagan Schoenholz and Zainab Yahya for their participation in data collection, data extraction, and quality assessment.
Footnotes
Competing interests: None declared.
Contributors: S. Pigeon, M. Lonergan, R.K. Pitman and A. Brunet designed the study. S. Pigeon and O. Rotondo acquired the data, which S. Pigeon, M. Lonergan, O. Rotondo and A. Brunet analyzed. All authors wrote the article, which S. Pigeon, M. Lonergan, R.K. Pitman and A Brunet reviewed. All authors approved the final version to be published and can certify that no other individuals not listed as authors have made substantial contributions to the paper.
Funding: M. Lonergan received a doctoral award from the Fonds de Recherche du Québec (FRQ-S). S. Pigeon received a master’s award from FRQ-S and from the Canadian Institutes of Health Research while working on this project.
- Received April 12, 2021.
- Revision received November 16, 2021.
- Accepted December 5, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.